How can building HVAC systems be modified to provide a safer environment in new and renovated spaces?
Learning Objectives
- Understand how the COVID-19 virus spreads through the air in buildings.
- Learn about airflow issues, and what mechanical engineers need to consider in occupied spaces.
- Review how ventilation and environmental standards (ASHRAE Standard 62.1 and 55, respectively) will be affected by the spread of the COVID-19 virus.
Indoor air quality has always been an engineering concern for building owners and managers and heating, ventilation and air conditioning designers and engineers. Engineering challenges are already omnipresent from ensuring adequate ventilation is maintained for maximum occupant comfort and productivity to avoiding the myriad complications from sick building syndrome and microbial contamination at the air handling units.
The current COVID-19 pandemic has put a new twist to the already multifaceted design challenges. Up to now, most HVAC contamination concerns have been located in a known location (e.g., outside air intakes, mold or other microbial growth in coil drain pans and drift carry-over into the ductwork) or a high concentration, like carbon dioxide, in the indoor ambient air that is not being effectively diluted.
With the SARs-CoV-2, commonly referred to as the novel coronavirus or COVID-19, the pathogen is highly lethal and can be spread by direct inhalation of respiratory droplets (5 to 10 microns and greater) and aerosols (smaller than 5 microns) from infected persons coughing, sneezing, talking, breathing or even shouting or singing. There are secondary transmission vectors related to contamination of HVAC system surfaces such as inside ductwork, coils, filters, motors and fans, which are a maintenance concern.
Complicating the situation, the infected persons are typically unknown to building authorities, are mobile throughout the building and the number of infected people in a given space are not known. On the face of it, the HVAC designer’s task to minimize the spread of the virus in the conditioned environment is incredibly daunting.
Our profession needs to go beyond our usual technical resources and start interacting with medical professionals, microbiology and virology scientists, scientists in specialized lighting systems, computational fluid dynamics specialists and others to better understand the fast-evolving research and formal technical guidance documents being published. This information is essential for HVAC engineers to understand how far the virus is spreading in the air and actually infecting others (e.g., droplets versus aerosol); how long the virus survives on various HVAC system surfaces as a function of temperature and humidity; what is the live viral load that makes it back through the AHU and recirculated through the supply air diffusers. The answers to these questions and concerns will contribute to effective solutions now and going forward.
This article addresses some of the direct concerns and solutions that have come up in the design of new and renovated spaces as well as secondary concerns regarding how some ASHRAE Standards may be affected by COVID-19 as it currently spreads unchecked in many parts of the U.S. and the world. The first part of the article addresses airflow issues in conventional office buildings, the second part discusses various technology solutions to help the HVAC designer and building owners, the third part addresses different building types like restaurants and fitness clubs; and lastly a brief review of some ASHRAE Standards and how they may be affected going forward as COVID-19 propagates across the globe.
Airflow issues
The problem with COVID-19 and ventilation is counterintuitive. With most inactive airborne contaminants like volatile organic compounds and carbon dioxide, we achieve an acceptable level of dilution to maintain an acceptable threshold limit for these common contaminants through prescribed quantity of outside air in the supply air based on occupancy or over time.
Generally, higher than code ventilation and overall airflow rates flush out contaminants in the occupied space more efficiently, though at greater energy usage versus code ventilation rates. For biological contaminants, specialized HVAC systems and room arrangements, e.g., positive and negative pressure isolation rooms, direct airflow from clean to contaminated and exhausted without recirculation in the space. The relative location of the patient and health care workers determine whether it’s an isolation or protection room. Most HVAC engineers understand this well.
The challenges with COVID-19 are twofold. First, aerosolized COVID-19 generally behaves like other airborne contaminants and tends to diffuse within a space and moves with air drafts. Unlike inactive contaminants however, repeated doses of exhalated virus being circulated throughout the space on drafts can infect people far away from the source. Although greater ventilation and airflow will dilute the concentration, they also increase recirculation of the virus in the breathing zone through drafts.
Second, unlike the negative or positive pressure isolation room described above, large numbers of unidentified, infected persons moving about freely in an enclosed space poses an immensely greater design challenge.
Before COVID-19, the free movement of people with a potentially deadly respiratory diseases were relatively rare in public spaces. Sick people were generally symptomatic before they were highly contagious and easier to identify and isolate through the public health system. Now, we are seeing that a majority of people who are COVID-19 infected and contagious are unknown, even to themselves and asymptomatic carriers. As such, the infection control isn’t occurring in an engineered health care facility isolation room.
Instead, we now have public spaces like office buildings, retail outlets, schools, restaurants and other public buildings that were never designed to control the person-to-person spread of respiratory virus laden air in the same space.
Additionally, the COVID-19 infected person is typically moving about freely within the public space. That makes the engineered removal of the airborne virus contaminants virtually impossible. To make matters even more complicated, the current research indicates there is a significant risk of spreading the disease through aerosolized virus particles which remain suspended in the occupied space.
Within all enclosed spaces, the first line of defense against the spread of the virus is wearing a face mask according to public health agencies like the Centers for Disease Control and Prevention and World Health Organization. Whether layered cloth, surgical or N95, masks specifically limit the spread of exhaled respiratory virus particles in droplets and even aerosol form. If a mask can significantly limit the release of the virus into the ambient conditioned air with negligible viral load, then there is very little concern the HVAC system will spread the airborne virus particles past the masks to adjacent or nearby people. Although this concept has been communicated clearly by health experts, there has been resistance due to external social factors that are causing a significant portion of the population from regularly wearing a mask in public. This is unfortunately causing the infection rate to explode across the country. Thus, we are back to engineers trying to come up with work arounds in public spaces.
Due to the variability of space layout and relatively high occupant density of conventional office spaces, the risk of spreading the infection can be very high. A problem with the majority of conventional office HVAC design and construction is that it assumes the only contaminants in offices are benign gases and particulates that can freely mix throughout the space and be diluted safely through a thorough mixing of the ambient air and fresh air in the breathing zone. The more the ambient air is mixed and replaced, the better the IAQ is assumed to be. Engineers aspire to design and have installed HVAC systems with no stagnant air pockets and a uniform temperature distribution.
To achieve that, engineers depend on traditional overhead office HVAC to take advantage of the coanda effect to have supply air hug the ceiling and gradually diffuse and drop as the airflow velocity drops to where the effect no longer exceeds the gravity effect on the colder, denser air and it drops to the occupied zone and offsets the heat sources of the space.
In perimeter zones, the distribution gets trickier due to the need to push air down along the perimeter fenestration and “curl” back up along the interior. That circular pattern is the start of problems in the post COVID-19 world. To identify the problem, let’s discuss how we currently know the virus to spread in enclosed spaces. The virus spreads from infected people through respiratory droplets and aerosol and the virus from these vectors can linger in the air for hours while larger droplets that precipitate can survive on some types of surfaces for days. Unlike in an engineered space like a health care isolation room, it can be spread by multiple people at the same time in an enclosed space with no specific dispersal pattern from the exhaled breath of mobile and static people.
Respiratory droplets are normally 5 to 10 microns in diameter. Plenty of research and guidance from the CDC and other public health agencies have established that these droplets fall to the ground fairly quickly and close to the source (within 1 to 3 feet) in still air. During a cough, these droplets can travel up to 6 feet from the source. During a sneeze, the smaller droplets can travel up to 10 to 15 feet from the source, depending on the severity of the sneeze, the person’s position, whether sitting or standing, and the geometry of the space. These distances have been modeled in computational fluid dynamics analysis and also physically documented by researchers.
The second type of particles people exhale are aerosols. These are very fine moisture particles typically 5 microns and much smaller in diameter. When these aerosols eventually evaporate, what is left are solid particles down to 0.1 micron called droplet nuclei. These particles are suspended in what one can typically see condensing into clouds when they exhale on a cold winter morning. Aerosols and droplet nuclei remain airborne for much longer and are easily carried far afield from the point of exhalation and diffuse by drafts from passersby and direct and induced drafts from HVAC supply diffusers and large return air openings. It is important to understand the size and concentration of the aerosol cloud leads to greater viral load contained in that volume of air. Combining with the larger droplets common in a cough or sneeze increases the viral load by two orders of magnitude.
The heavier droplets generally are not as susceptible to HVAC system drafts. However, aerosols and droplet nuclei naturally diffuse from high concentration to a local equilibrium and distributed throughout the space by HVAC drafts.
According to Lydia Bourouiba, Ph.D., referring to the discharge trajectory from a sneeze, “Droplets that settle along the trajectory can contaminate surfaces, while the rest remain trapped and clustered in the moving cloud. Eventually the cloud and its droplet payload lose momentum and coherence, and the remaining droplets within the cloud evaporate, producing residues or droplet nuclei that may stay suspended in the air for hours, following airflow patterns imposed by ventilation or climate-control systems.”
Keep in mind that most research literature indicating the normal travel distance for droplets and aerosols from normal breathing and speaking (approximately 6 feet), coughs (approximately 6 to 15 feet) and violent, unrestricted sneezes (up to 20 feet or more) are based on still air, defined as air movement less than 20 feet per minute. Overlaying with horizontal HVAC system drafts from 50 to150 fpm drastically increases these distances in the direction of the HVAC system draft.
Although the HVAC system can contribute to the spread of the aerosols, it also provides the fresh air that will dilute the concentration of suspended virus particles in the air. It is this dichotomy that is the engineer’s challenge. How do we ensure the introduction of fresh air from supply diffusers does not inadvertently distribute virus-laden air from one person to the next and beyond in an open plan layout such as open offices and large meeting rooms and extending to restaurants, retail shopping, etc.?
Conventional air movement in commercial office spaces with lay-in ceilings tends to travel horizontally along the ceiling and then slowly drops down (see Figure 1). This airflow pattern minimizes the likelihood of spreading contaminated air from one person to adjacent people as the majority of the horizontal movement is well above the breathing zone.
Air movement in the breathing zone is typically very low velocity-induced air combining primary conditioned air with ambient room air. Increasing air changes would reduce the virus concentration in the space, but that increased airflow, if not accounted for with proper diffuser/neck size selection, also has the potential to spread the virus if drafts intersect and primary airflow in the breathing zone becomes more horizontal than vertical.
Some recent ASHRAE COVID-19 guidance has suggested increasing the outside air percentage through the air handling system. It is true that greater supply air to the space will dilute the concentration of airborne viral aerosol and droplet nuclei in the space.
However, unless research and testing can prove aerosols and droplet nuclei are being drawn back to the AHU and recirculating back into the space, increasing outside air percentage through the AHU will not dilute the virus in the conditioned airstream because the AHU system itself is not the source of the contaminant. Unlike CO2 from occupant breathing, which can be easily measured in the return airstream to prove it is reintroduced to the occupied space if not diluted with outside air, it is not a given that high viral load infectious aerosols and droplets are being entrained in the return air stream and recirculated back through the HVAC system as live virus in concentrations to cause likely infection.
Because the contaminant source doesn’t originate in the HVAC system like mold or Legionella and it isn’t suspected to be drawn back to the AHU as live virus in any significant quantity, it isn’t likely to be distributed through supply ductwork. The droplets are too heavy to get drawn up into the return ducts and the aerosols are getting diffused and precipitating in the occupied space, or at most precipitating in return air plenums and ductwork, if they even make it up that high. Any larger aerosol that may get to the AHU will likely attach to wet coils and filter media.
There needs to be much more research on how many live virus particles make it into the return ducts and then through cooling and heating coils, filters, etc. Unlike molds and other fungi that can go dormant and spread spores that can propagate once conditions are suitable months or years after, dead viruses remain so and are of no concern. If the presence of live virus in the HVAC system is high and sustained, even the regular removal of filters and equipment maintenance will require significant service technician personal protective equipment and proper disposal.
However, it is the author’s opinion that the concentration of live virus in the return airstream is negligible and those in the supply airstream are even lower, if not nonexistent. However, this needs to be validated with laboratory or infield testing.
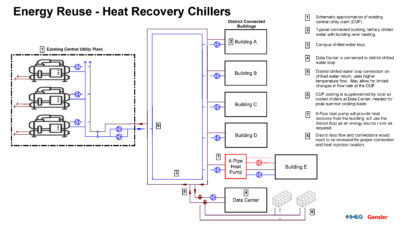
To minimize the spread of the COVID-19 virus in a mechanically ventilated space, the air distribution has to be more like an isolation room with only one pass across the breathing zone. Because we don’t know who’s infected, there’s no practical place to return the air like at the head of the patient bed in an isolation room. In light of that, one approach is to setup an inverted underfloor displacement ventilation system.
In a conventional underfloor displacement ventilation system, supply is released down low (typically floor diffusers) in the occupied zone and returned up high where the hot air is out of the occupied zone. With COVID-19, the optimal system has air dropping straight down at low velocity to minimize blowing respiratory droplets and aerosols horizontally toward adjacent people and complementing gravity to draw down contaminated air toward the floor and eliminating aerosols from being drawn back up through the breathing zone (see Figure 2).
This is an expensive solution in new or totally renovated spaces and the height of the raised floor needs to minimized to allow short ramps or other adjustments to account for the change in floor height. Alternately, the return air can be routed through floor openings to the ceiling cavity below and ducted back to return air shafts. This is a relatively easy solution that only shifts the return air to the floor below, but otherwise doesn’t drastically change the building air handling system.
Either approach does require significant buy-in and coordination with architects and building managers. However, this approach does significantly reduce the likelihood of cross-contamination of clean supply air and contaminated breathing air in the occupied zone. An alternate approach for existing spaces that still minimizes cross-contamination is to put return air chases in walls and partitions with return air slots near floor level.
Technology solutions
Within occupied spaces, there are emerging technologies that allow neutralizing the COVID-19 virus particles in the air and on surfaces. Ultraviolet-C lights (particularly tuned to 254 nanometer wavelength) have been shown to effectively inactivate the virus in the ambient air space and on surfaces in a relatively short time depending on the intensity.
However, this particular wavelength of UV light damages human skin and corneal tissue and cannot be used while the space is occupied by people or animals. Care must be used to block glazing that may allow the light to escape beyond the room being treated and affect people. This type of lighting is common and effective within AHUs to kill mold, pathogens and algal growth on condensate drain pans. They are also installed in commercial kitchens and laboratories, but require warning devices to keep people and animals away from direct UV light exposure.
Research by a team at the Columbia University Medical Center has shown that far-UVC light — ultraviolet light from roughly 200 to 222 nm wavelength — is effective at inactivating most viruses, including coronaviruses, while not damaging human skin or corneal tissue when limiting exposure (combination of light intensity and exposure duration) withing tested limits. The evolving application of this new, safer light source is to disinfect the occupied space air when it is being occupied to provide a safer environment for occupants. Their research has been incorrectly referenced in some manufacture’s literature, so engineers need to be diligent in doing their own reading and research to make sure products do what they claim and ensure the application is actually providing the intended disinfection safely.
The primary concern for professional engineers where far-UVC lights are specified is to make sure the intensity of the Far-UVC lighting system is appropriate for the expected maximum duration of exposure by individuals. The University of Rochester has a website that summarizes acceptable exposure limits. Their website states, “There is no Occupational Safety and Health Administration standard for exposure to ultraviolet light, but the National Institute for Occupational Safety and Health recommends that the time of exposure to an intensity of 100 microwatts per square centimeter at wavelength 254 nanometers not exceed one minute. When averaged over an eight-hour workday, this value is 0.2 microwatts per square centimeter.”
Currently, there is no differentiating OSHA or NIOSH guidance for 222 nm UVC light exposure limits versus 254 nm UVC light. The University of Rochester website also states that lighting in the UVC range (100- to 280-nm wavelength) generates ozone in the treated space. Some ASHRAE documents also cite this concern of ozone production, but primarily at wavelengths below 200 nm.
In general, selecting lights ranging between 207- to 222-nm, but biasing toward 222-nm, appears to be optimal. The University of Rochester website also indicates “The American Conference of Governmental Industrial Hygienists has issued threshold limit values for occupational exposure to UV” lighting.
Specifying engineers should be aware of these threshold limit values before specifying products used in occupied spaces.
The advantage of far-UVC lighting is that it can disinfect the occupied space while it is occupied, minimizing the viral load in the occupied space. According to research by the Columbia University team, maintaining regulatory exposure limits, exposure time to effectively inactivate virus particles ranges from roughly eight minutes for 90% inactivation to around 25 minutes for 99.9% inactivation. This is very important to note.
Many manufactures of 254 nm UVC lights offer products that can be installed in ductwork or AHUs. The specifying engineer has to verify the actual wattage of the fixture, intensity across the full width of the airstream, and most importantly, the required duration at that intensity to provide meaningful inactivation of airborne virus particles. Humans are not in the ductwork or the AHU, so surface disinfection of ductwork or AHUs is not the goal. Any installation in HVAC equipment should be for the purpose of inactivating airborne virus that may be shunted through the system and discharged through supply diffusers in any significant quantity.
Knowing that the velocity of air traversing through ducts and AHUs, the exposure time within 2 feet of the light (4 feet total length) is 2/3 of a second at 400 fpm typical in an AHU to 0.16 seconds at 1,500 fpm common in ductwork. The effectiveness of these devices in that application are questionable at best as most of these lights require sustained exposure for minutes, not fractions of seconds. Even the use of 222 nm UVC lighting needs to take into account the intensity and safe exposure duration and also the time required to inactivate live virus.
Also, it should be noted that UVC lights only sanitizes the surfaces the light touches within a defined distance to maintain intensity. If the room has overhead UV germicidal irradiation lights, the underside of tables and chairs and backsides of furniture away from the lights are not exposed to the UVC lights and will not be sanitized. Ceiling-mounted UVC lights lose intensity at an inverse squared ratio the farther away the surface is.
Therefore, multiple lights at a fairly close spacing will be required for specified effectiveness. Areas blocked from the UV light source by suspended ambient light fixtures, exit signs, signage or furniture or partitions at lower levels should be minimized. Careful coordination is required to reduce these blind spots. As important as exposure on surfaces is, the specifying engineer also needs to consider the exposure on occupants.
With the 0.2-µW/cm2 threshold for an eight-hour shift guidance, it is important to verify that the system layout does not exceed that and ideally is slightly below that to ensure that occupants who are standing most of the time are closer to the light source and get a significantly higher exposure than people seated.
One other class of equipment engineers should consider are in-room recirculating filters. These filters operate similar to a side-stream filter in a hydronic system. They remove virus particles from the air around it, thus reducing the overall viral load within the occupied space. The in-room filters are typically portable, plug-in type units with a small blower and a high-efficiency particulate air filtration unit.
It is important to select a unit that takes air in from the top and diffuses the clean air out the bottom or bottom sides. Units that discharge the air from the top can inadvertently blow virus-laden air in its discharge path to other occupants further away. These units are especially effective in small rooms such as medical and dental exam rooms. These units are pressure neutral to the space, so a separate room exhaust fan is still required to maintain negative pressurization in rooms where a known or suspected infectious person is present.
Another technology that is being heavily presented to engineers is air stream bipolar ionization. While manufacturers are making significant claims of their efficacy, neither ASHRAE nor the CDC have a direct position on the technology.
From ASHRAE’s website summarizing CDC’s position, “While bipolar ionization has been around for decades, the technology has matured and many of the earlier potential safety concerns are reportedly now resolved. If you are considering the acquisition of bipolar ionization equipment, you will want to be sure that the equipment meets UL 2998 standard certification (Environmental Claim Validation Procedure for Zero Ozone Emissions from Air Cleaners), which is intended to validate that no harmful levels of ozone are produced. Relative to many other air cleaning or disinfection technologies, needlepoint bipolar ionization has a less-documented track record in regards to cleaning/disinfecting large and fast volumes of moving air within HVAC systems. This is not to imply that the technology doesn’t work as advertised, only that in the absence of an established body of evidence reflecting proven efficacy under as-used conditions, the technology is still considered by many to be an ‘emerging technology.’”
The CDC leaves this commentary with the caveat, “Consumers should research the technology, attempting to match any specific claims against the consumer’s intended use. Consumers should request efficacy performance data that quantitively demonstrates a clear protective benefit under conditions consistent with those for which the consumer is intending to apply the technology. Preferably, the documented performance data under as-used conditions should be available from multiple sources, some of which should be independent, third party sources.”
Building managers turn to consulting engineers as a trusted source for proven, cost-effective solutions. As such, it is imperative for the consulting community to do its own due diligence and homework to review third-party, independent research validating any performance claims.
Space-specific applications
Designers must be aware of different air distribution approaches common in restaurants, bars, showrooms, gymnasiums, health clubs and similar spaces with open ceilings and suspended or soffitted supply ductwork with sidewall air diffusers (see Figure 3). These types of spaces with supply airflow drifting predominantly horizontally are of primary concern in the person-to-person transmission of the COVID-19 virus.
Whether from above or even sidewall or window air conditioning units in smaller cafes and diners, existing facilities should have the airflow redirected up as high as possible to keep high-velocity horizontal throw well above the breathing zone, allowing the air to diffuse and slow before dropping into the breathing zone and causing minimal draft. In new facility design, this standard design approach must be modified to minimize the horizontal airflow movement in the breathing zone. This holds true for gymnasiums and health clubs as well, where direct horizontal airflow to provide convective cooling is common.
ASHRAE 62.1 and 55
Whenever discussions revolve around airflow and ventilation, ASHRAE Standard 62.1: Ventilation for Acceptable Indoor Air Quality and ASHRAE 55: Thermal Environmental Conditions for Human Occupancy always should be reviewed for their relevance to the discussions. Both of these standards have a direct interaction with regard to the factors controlling the dilution of the virus in the occupied space and how the air distribution in the space affects inadvertent spread of the virus from one person to others around them.
Looking at ASHRAE 62.1 first, it is useful to review the intended purpose and scope of the standard relative to the spread of an infectious respiratory virus. Section 2 describes the scope of the standard and states in subsection 2.6, “Ventilation requirements of this standard are based on chemical, physical, and biological contaminants that can affect IAQ.”
Pertinent to the current situation, subsection 2.8 states, “This standard contains requirements in addition to ventilation, related to certain sources, including outdoor air, construction processes, moisture and biological growth.” The standard defines IAQ as, “air in which there are no known contaminants at harmful concentrations as determined by cognizant authorities and with which a substantial majority (80% or more) of the people exposed do not express dissatisfaction.”
Reviewing these passages, the standard clearly has jurisdiction of specialized conditions to mitigate the spread of COVID-19 virus within buildings based on the stated purpose and subsection 2.6 of the scope of the standard. Knowing the lethality of the COVID-19 virus and the anonymous spread of the virus through regular respiration, all air within each occupied space appears to now fall under the most severe classification, Class 4, which is defined as “Air with highly objectionable fumes or gases or with potentially dangerous particles, bioaerosols or gases, at concentrations high enough to be harmful.”
There may be some argument that the passage about “… concentrations high enough to be harmful …” may not apply to this situation. Some may even try to argue that this does not apply to an office environment where generally sedentary activity may not create an environment where enough viral load is being exhaled in such force as to spread the droplets or aerosol beyond an individual’s personal space.
However, because the prevalence of asymptomatic, infected and contagious persons is being reported in the news media to be very high, the only defensible design assumption has to be that building spaces must be treated as if all occupants are COVID-19 positive. If designers accept that all indoor air in occupied spaces is now to be treated as Class 4, that changes the fundamental operations of all buildings. The majority of commercial building AHUs do not have the cooling and heating capacity to be converted to 100% outdoor air units.
Compounding this dilemma, even if designers can convert all systems to 100% outside air with direct exhaust from each space, it still does not, on its own, address the spread of the virus from person-to-person within a given space. Yes, there is dilution of the viral load with a space, but doesn’t the movement of air within the space itself cause the spread of the virus?
Additionally, it is not certain or even likely that the virus in concentrations that will make a difference, returns to the AHU and then gets recirculated back to the occupied space. If it isn’t proven that the virus successfully recirculates, there’s little benefit in the energy penalty of 100% outside air units or even higher than current minimum ventilation rates in ASHRAE 62.1-2019, Table 6.2.2.1, Minimum Ventilation Rates in Breathing Zone.
In the only space a similar situation previously existed, hospital isolation rooms, the air distribution system is specifically designed to minimize the spread of the infections exhalation of a known infected person by drawing clean, outside air across the room, washing health care workers with clean air as it is drawn to the infected patient and exhausted as close to the patient’s head as practical.
In the new normal of COVID-19, the infectious patient is anonymous, mobile and numerous. Beyond wearing masks to minimize the spread of the virus at the source, it does not seem there is any simple, quick and cheap solution. At a minimum, personal desk fans that can blow ambient air from one cubicle to another should be categorically removed. As suggested above, the inverted displacement ventilation model with return/exhaust down low at floor level, though not cheap, does provide a credible means of minimizing the spread of the virus.
The addresses some of the basic design concerns and solutions in new and renovated spaces as well as a brief review of how ASHRAE 62.1 may be affected by the pandemic as it currently spreads unchecked in many parts of the U.S. One of the most effective solutions is ultimately the simplest — wearing a mask. Although a vaccine may offer some relief to the COVID-19 pandemic, the global spread of the virus to every corner of the planet occupied by humans will ensure mutations with similar lethality will certainly evolve and the cycle will begin again.
Where previous respiratory diseases like SARS and MERS were manageably confined to a region without global spread, it is likely that mutations of the current COVID-19 virus, which has established a foothold on every continent except Antarctica, will now spread much more readily across the globe. The much feared normal of global viral pandemics may be upon us. It is another health care and engineering challenge along with climate change.