A hospital’s air handling system had to be reconfigured so that pressurization remained at the correct levels
A Midwestern community hospital recently experienced problems with its surgical suite in that some of the operating rooms were flipping back and forth between being positively pressurized and being negatively pressurized. This was occurring during both occupied and unoccupied hours during all seasons of the year.
This was a significant problem for the facility because ORs must be positively pressurized at all times, even when the rooms are unoccupied, to limit the introduction of airborne contamination into the OR. After retesting the supply and return airflow rates for each operating room and adjusting flow rates back to their design values, they were dismayed to find out that the problem still persisted.

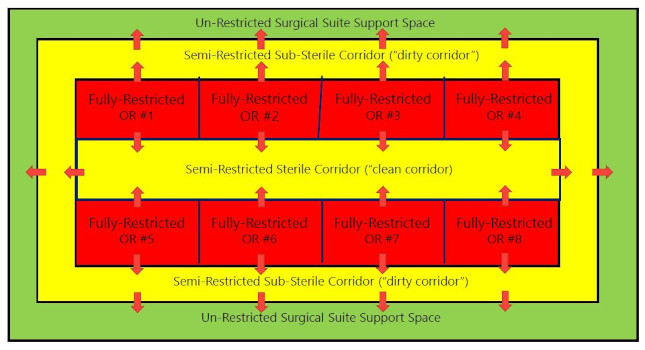
The investigation began by reacquainting the owner with exactly how a surgical suite should be pressurized — at both the OR level and at the suite level simultaneously.
Note that the ORs, which are defined as restricted areas, must be positive to the spaces around them, which includes the semi-restricted corridors (both clean and dirty corridors). The restricted corridors, in turn, must be positive to the unrestricted department around them. This cascading pressurization is critical to both contamination control and, ultimately, to infection control.
The overall heating, ventilation and air conditioning system was configured such that the ORs, the sterile corridors and the sub-sterile corridors were all serviced by the same air handling system. The supply air ductwork had terminal units with reheat coils used to control airflow and pressurization.
However, the return air ductwork was designed and built as a low pressure, pressure-dependent sub-system, meaning it didn’t have any terminal units. This resulted in airflow control and pressurization being determined strictly by the tracking of the supply and return air fans back in the air handling unit.
In addition, the location of ceiling-mounted supply and return air diffusers in the sterile and sub-sterile corridors was less than ideal. The ceiling-mounted supply air diffusers in both the sterile and sub-sterile corridors were installed directly adjacent to the doors to the ORs. This resulted in the supply air delivered directly outside the ORs, pushing into the ORs directly against the air that was trying to be pushed out of each OR to keep it positively pressurized.
This air pressure battle phenomenon was occurring during full occupancy, partial occupancy and unoccupied modes. Moreover, because there were no terminal units in the return air ductwork, there was no direct control over much how much return air was being moved through any ductwork at any point in time anywhere within the restricted areas. These two factors created enormously varying differential pressures between the corridors and the ORs, resulting in the ORs flipping to negative pressurization from time to time.


How did the HVAC engineering team rectify this situation in a functioning surgical suite?
Step 1 was to reconfigure where the ceiling-mounted supply and return air diffusers were installed in both the sterile and sub-sterile corridors. It was decided that the return air diffusers should be relocated just outside the OR doors to help reinforce air exfiltration out of the adjacent OR. The supply air diffusers in both the sterile and sub-sterile corridors were relocated closer to the perimeter of both sterile and sub-sterile corridors such that they could positively pressurize those corridors with respect to all the building areas outside the surgical suite itself.
Step 2 was to furnish and install terminal units in the return air ductwork to convert that system from a pressure-dependent system to a pressure-independent system. This subtle but important feature of an air handling system must be considered during the initial planning of the system so that both the AHUs and the companion duct distribution work together as a system to achieve the desired pressurization criteria.
Providing the new return air terminal units allowed both the supply and return air flow rates in both the sterile and sub-sterile corridors to be established and maintained to achieve proper pressure balances in the surgical suite over the life of the building. In other words, the ORs need to be positively pressurized with respect to the sterile and sub-sterile corridors at all times. In addition, the sterile and sub-sterile corridors need to be positively pressurized with respect to the building areas outside the surgical suite.
The modifications made to the supply and return duct distribution systems helped resolve the OR pressurization problems as borne out by subsequent testing and balancing work, commissioning work and ongoing monitoring of both airflow rates and room pressurization.