With daunting aspects such as ever-changing codes and standards, increasing medical complexity, and dwindling capital budgets, hospitals and health care facilities are among the most challenging building projects.

Neal Boothe, exp Global Inc., Maitland, Fla.
David W. Crossey, Principal/Vice President, Lovorn Engineering Assocs. LLC, Pittsburgh
Jeff Harris, PE, LEED AP, Director of Mechanical Engineering, HGA Architects and Engineers, Minneapolis
Michael McLaughlin, Senior Vice President, Southland Industries, Washington, D.C.
Michael Sheerin, PE, LEED AP BD+C, Principal, Director of Health Care Engineering, TLC Engineering for Architecture, Orlando, Fla.
CSE: What unique requirements do HVAC systems in hospitals have, and how have they changed in the past one to two years?
McLaughlin: The continued push to reduce energy consumption by HVAC systems in hospitals is leading to more innovative designs. Developments that are influencing designs decisions today include the energy reduction goals set in motion with the Energy Policy Act of 2005, the Energy Independence and Security Act of 2007 (EISA), and related executive orders. Current solutions include a wide range of modified or new mechanical systems as well as the effective yet costly solution of PV arrays. This is certain to change as academic institutions, engineers, and manufacturers work together to create new solutions that will meet the challenge.
Crossey: Minimum air changes, minimum outside air requirements, and the capability to maintain specific humidity levels are definitely unique to hospital HVAC systems. I don’t believe the changing requirements have affected the design process, but the HVAC systems are being looked at more closely by the code reviewers and infection control professionals.
Sheerin: The biggest change over the last few years is that changes in the energy code and the stretch goals of higher LEED points that we often target with our hospital clients have necessitated that we pursue a lot more avenues and strategies in achieving greater energy efficiency. These are great things, but you still have to make it understandable and embraceable by the operating staff. They have to be the champions for wanting it to work.
Harris: Fully ducted supply and return systems are required for hospitals; some developers are surprised by this. While not always a formal requirement, owners are requesting that the hospital’s cooling system be capable of operation during an electrical outage and that the cooling system redundancy be reviewed. There is a relatively recent trend regarding the owner’s request for providing a negatively pressurized operating room in the OR suite for infectious patients. For systems serving areas such as surgery, which have traditionally operated at full volume continuously, the design team is being asked to find a control scheme that reduces the energy consumption. Older systems that had been constant volume are being changed to two-position systems that switch to the minimum airflow setting when not in use. New systems are designed with two-position constant volume supply boxes with tracking constant volume return boxes, to maintain pressure relationships at full volume and at reduced volume. This is being enhanced with actually tracking the usage of the room itself based on when the patient is scheduled to enter and when time of departure is anticipated. This will provide even more energy savings as the rooms are being monitored more closely and not operating at a higher level than needed. How the hospital makes use of the system turndown capability requires extensive discussion and agreement between the design team, the hospital facilities team, and the hospital’s professional staff (doctors, nurses, and administration). Expected hours of operation, the ability to clean and turn around an operating room, and how the room is cleaned all play into the amount of time the operating room is at full volume and when it can run at reduced volume.
CSE: How do you apply ASHRAE Standard 170, Ventilation of Health Care Facilities, to infection control systems in hospitals?
Harris: At a minimum, following the required minimum air change rates and pressure relationships. The pressurization requirements can create paradoxical situations. One of our clients recently had an inspector request that the clean corridor (outside the operating rooms) be positively pressurized to the operating rooms, since his interpretation was that sterile supplies were temporarily stored in the corridor and therefore the corridor was “sterile storage” and required to be positively pressurized, as are operating rooms. This request resulted in a number of discussions with the hospital’s infection control staff, the hospital’s facilities staff, and the design team.
McLaughlin: ASHRAE Standard 170 provides a number of prescriptive measures related to infection control, such as air change rates, pressurization, air filtration, and moisture control, among others. The application of infection control on a much broader scale is often the result of informed engineers moving beyond prescriptive requirements. Once case in particular is the choice between conventional recirculating air systems or 100% outside air systems. Although little research or empirical evidence exists related to the transmission of airborne infectious disease through the HVAC system, there is a contingent of designers that believe 100% outside air systems, when coupled with the appropriate technology and energy-reducing features, offer significant benefits that improve the safety of the indoor environment for both patient and staff, reduce the initial investment and long-term operating costs, minimize facility maintenance, and improve the flexibility of the hospital. I am a significant proponent of this approach, and our company has designed numerous, award-winning hospitals across the country using this concept. Our driving purpose is to maximize the safety and indoor environment for the benefit of both patient and staff.
CSE: Keeping recent outbreaks of Legionellosis (Legionnaires’ disease) and Pertussis (whooping cough) in mind, what are hospital clients requesting to help ensure patient safety?
Sheerin: There is a lot of planning to address any worst-case scenario affecting an emergency department, and we have assisted some hospital clients’ plans for operating a patient wing or floor in a “surge” mode with all-in/all-exhausted airflow. Each hospital is unique in the issues and concerns it has, so you really need to discuss and develop the best plan with its needs in mind.
Crossey: Existing central AHUs are being scrutinized for their part in making the building environment safe. Undesirable organisms may thrive in older equipment due to moisture buildup within the units or growth on coils. We have been involved in the replacement of several AHUs recently and we have been replacing the coils and adding UV lights to maintain internal cleanliness. We have also started to add moisture sensors in drain pans to alert the maintenance staff of potential problems.
Harris: In new construction, we design the waiting area and adjacent exam areas to minimize the number of AHUs that an infected patient might walk through. Keeping waiting areas negatively pressurized is important. More clients are interested in providing ultraviolet lights in the AHUs, both for infection control and improved heat transfer at the cooling coils.
McLaughlin: With regard to Legionellosis, basic requests are eliminating water storage, or when storage is desired, maintaining a minimum 140 F water temperature. Other side-stream systems such as copper-silver-ionization have been desired by our clients.
CSE: Have low-flow plumbing fixtures become the norm in your hospital projects? Why or why not?
McLaughlin: Low-flow fixtures have become more common in health care projects to meet the sustainability goals of the project. Their use is limited to certain applications as patient safety, codes, and standards can take precedence.
Sheerin: Absolutely. Regardless of LEED, hospital owners see the benefit and know how much water they are saving, and what an easy cost benefit that is for them.
Harris: Yes, for the public toilets. Patient rooms and procedure rooms are often not low-flow fixtures. Some facilities have experienced maintenance problems with low- or no-flow fixtures.
Crossey: We specify low-flow water closets, showers, and faucets. Most of these selections are dictated by code; however, our standard specifications are based on water-saving devices. They work well and they save water, which in the end saves our client money.
Boothe: Hospitals recognize that low-flow plumbing fixtures can reduce water and energy consumption and provide a sterile environment. Increasingly, low-flow fixtures are designed to meet the high-volume and infection-control needs of the hospital while providing water and energy savings. Designers should specify low-flow fixtures for public spaces while investigating the range of products available that operate on-demand for patient rooms, nursing stations, operating rooms, and foodservice preparation. Dual-flush toilets and low-flow shower systems are appropriate in patient rooms.
CSE: Discuss chiller and/or boiler plants in a project you recently worked on.
Harris: Over the last two or three years, we have worked on three different Virginia central plant projects that encompass biomass boilers or cogeneration of electricity and steam. For our continuing clients, we have recently completed three expansions of central plants, changing primary/secondary chilled water systems to primary pumping only, and upgrading and improving the control and energy efficiency of the plants.
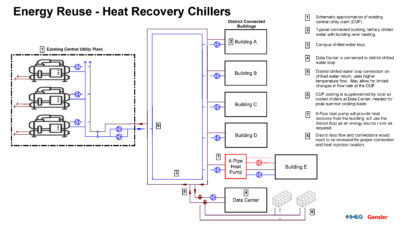
McLaughlin: Given the continued strive to reduce energy use in health care facilities, chiller and boiler plants are undergoing a transformation. Energy-reducing features such as optimized chilled water and condenser water temperature, split (sensible and latent) chilled water plants, heat recovery chillers, geothermal applications, and new chiller technology are being used to reduce total energy consumption. Similarly, the boiler plant continues to evolve to include limited or distributed steam production, reduced and optimized hot water temperatures, and the integration with heat recovery chillers, geothermal applications, condensing boilers, and lifecycle cost evaluations of heat recovery options. Each project is unique and provides an opportunity to mix, match, or even create new solutions to achieve the cost and energy performance goals of each project.
Crossey: We recently completed an upgrade to the chilled water plant at Ruby Memorial Hospital in West Virginia. The project was phased over several years due to budget constraints; the final system capacity was 4,200 tons. The existing chilled water system consisted of two 750-ton chillers (1988 vintage) located in the original building and two 600-ton chillers (2005) located in the northeast addition. We added three new 1,000-ton variable speed chillers to the existing mechanical room along with new variable speed primary and secondary pumping. We also needed to add three roof-mounted cooling towers with new condenser pumps and an extensive roof grillage system for maintenance. The new plant controls and the revisions that were made to the control sequences resulted in a substantial reduction in energy usage.
Sheerin: The Nemours Children’s Hospital is a project that we were delighted to design, and the hospital has a truly unique hybrid heating system that allows it to generate heating water via three means: a heat pump chiller, high-efficiency condensing boilers, and/or a heat exchanger coupled to 100/200 bhp flextube boilers. This happened for a lot of reasons, but it has given the Nemours folks tremendous flexibility and strategies for redundancy and exploring energy optimization of their heating plant. They just completed construction and it runs better than we imagined.