Air handling units are central to most HVAC systems in all nonresidential building types. This article looks at the codes/standards that define correct specifications and outlines best practices for calculating an AHU's requirements in a health care facility.
Learning Objectives
- Learn how to select the right type of air handling units (AHUs) for a health care project.
- Consider budget considerations when designing and specifying AHUs.
- Understand the different sections of the AHU and how they should be specified.
Air handling units (AHUs) are the most common means of air distribution in nonresidential buildings. AHUs are used to provide the airflow required for ventilation, heating, and cooling. AHUs in a health care setting are very important because they provide the required air change, filtration, and ventilation requirement to minimize the spread of airborne infectious diseases.
The mechanical engineer is responsible for the design and selection of AHUs for the critical spaces in a health care facility. Designing air distribution systems to serve hospital environments is a complex undertaking. There are specific requirements for ventilation and filtration to dilute and reduce contamination in the form of odor, airborne microorganisms and viruses, and hazardous chemical and radioactive substances.
Ventilation effectiveness is very important to maintain appropriate indoor air quality for patients and to minimize the risk of airborne hospital-acquired infections (HAI). There are additional design sophistication elements for the AHUs to minimize the risk of transmission of airborne pathogens and preserve a sterile and healing environment for patients. Choosing the right AHU plays a key role in minimizing HAI because the quality of the outside air and filtration effectiveness is controlled by the AHU design.
Several questions must be answered before the selection process begins. Some of the items are not unique to health care facilities and can be applied to most AHUs that serve high-performance buildings. Consider:
- What type of spaces will the unit be serving?
- What is the available budget?
- Where will the unit be located?
- What is the performance requirement?
- What is the filtration requirement?
Health care spaces
The spaces served determines the type of AHU selected. Health care spaces can be separated into critical and noncritical environments. The critical environments, such as operating rooms (ORs), intensive care units, post-anesthetic care units, neonatal intensive care units (NICUs), airborne infection isolation rooms, and protected environment rooms, will require an AHU that will provide the required ventilation per ASHRAE Standard 170-2017: Ventilation of Health Care Facilities. These units usually include added components like humidifier sections and filtration using high-efficiency particulate air (HEPA); in some cases, such as in ORs, it is considered good engineering practice.
Noncritical environments, such as general exam rooms, provider offices, general laboratories, and general patient rooms, do not require HEPA filtration and humidification. When selecting AHUs for health care spaces, the engineering best practice is to separate the units that are serving critical spaces from noncritical spaces.
Budget constraints may sometimes dictate that separate units maybe cost prohibitive, and for these instances, the AHU should be selected to meet the more stringent ventilation requirements of all the health care spaces that are served by the single unit. Alternatively, separate the ductwork for critical and noncritical spaces from a common AHU and provide the more stringent (i.e., more costly in first-cost and operations) spaces with duct-mounted supplementary systems.
Filtration requirement
There are several guidelines that govern filtration requirements for licensed health care facilities. These facilities, for one, are required to comply with the guidelines of The Joint Commission. Regarding filtration requirements for health care facilities, The Joint Commission references the Facility Guidelines Institute (FGI) Guidelines for Design and Construction of Hospitals, 2018 edition (which, in turn, references the ASHRAE Standard 170, 2017 edition, for the requirements governing filters for all areas within a health care environment).The FGI Guidelines for Design and Construction of Hospitals, 2018 edition, stipulates that all areas of inpatient care, treatment areas, and diagnosis—as well as those areas providing direct service or clean supplies, such as sterile and clean processes—should contain two levels of filtration. The first level is a pre-filter that meets the 2017 edition of ASHRAE Standard 52.2: Method of Testing General Ventilation Air-Cleaning Devices for Removal Efficiency by Particle Size MERV rating of 8 (MERV 8). The second level requires a final filter that meets the ASHRAE 52.2 MERV rating of 14.
The first filtration bank is MERV 8 pre-filter and should be located upstream of all the coils; these are usually panel-type filters. The final filter for a standard AHU without HEPA should be downstream of all the fans and coils, per ASHRAE 170. Some health care facilities will install HEPA in AHUs serving operating rooms; this HEPA filter should be placed downstream of the coils and fans and can be in the ductwork.
Budgetary considerations
Most commercial building projects are designed with a prescribed budget that will dictate the decision that the engineer makes in their AHU section. AHUs can cost anywhere between $4 to $12 per cubic feet per minute (cfm). If there is a cost constraint, packaged rooftop units (RTUs) will be selected because of the low cost. These units are often selected when there is not a central plant available, typically for use in medical office buildings, assisted living facilities, and outpatient surgery centers.
These package units generally contain fan sections, cooling coils, heating coils, filters, and dampers in a single casing. Humidifier sections can be added if a stringent humidity band is required in the health care space. Often, the casing includes its own air conditioning compressors and means for heating, such as gas burners, electric heating coils, and heat pump refrigerant coils. It is important to note that these units may have the lowest efficiency and are maintenance-intensive. Of course, there are some RTUs that have premium efficiency, but they do come at a higher cost than the standard RTUs.
The next tier of AHUs that are selected for health care spaces, if the budget allows, are modular AHUs; these units allow engineers to select individual components contained in modules having similar construction and cross-sections. The engineer can select the type and thickness of casings, supply fans, return fans, filters, coiling coils, heating coils, humidifiers, and other accessories. These units usually are called off-the-shelf units because the modules are fixed and cannot be customized to the level of a custom AHU. The units are either assembled by the manufacturer or can be taken apart and shipped in sections and assembled onsite. These units are generally more energy-efficient than package units and allow greater flexibility with location and orientation.
The next tier of units used in health care facilities are custom AHUs. Custom units are available in any configuration that the project may require. They usually have the highest-quality construction. They are sometimes necessary because of the space constraints at some health care facilities. They are often used in health care renovation projects where the replacement of units needs to meet very tight space requirements.
The units can be configured to include almost any combination of air-processing components. They can be specified to include service areas within the unit and can even accommodate pipes and equipment, like pumps or heat exchangers in a penthouse-type unit. They are more expensive than standard RTUs and modular AHUs, but they have a lower leakage rate and longer life because they are usually specified with higher-quality components (see Table 1).
Field-erected AHUs also are used in health care facilities. These units are specified in the same way as custom AHUs, but the final assembly of the units occurs onsite and is usually done by the mechanical subcontractors instead of the unit manufacturers.
These units’ performance and energy efficiency are not guaranteed because they are not tested in the factory environment. However, if assembled properly, they can be field-commissioned to have a high level of performance. These units are not often specified in health care design because their performance depends on the skill level of the contractor assembling the unit. Best engineering practice suggests that factory-assembled units are usually more reliable and have better performance. These units may have a higher final cost than all the other units because of the variations in field-installation costs.
Fan selection
When specifying an AHU for health care facilities, the fan type and arrangement is the most critical to ensure a high level of performance. There are many types of fans available; the main differences among them relate to blade configuration and the location of the fan wheel, whether it is fully housed or open. An open-wheel configuration is known as a plenum fan.
Selecting the right type of fan and the right fan size is important because this usually determines the energy efficiency, acoustics, and cost. A plenum fan consists of a centrifugal fan wheel without the surrounding housing. The fan wheel pressurizes the surrounding plenum, allowing air to discharge in multiple directions. Most health care facilities are increasingly using plenum fans as the preferred fan option for their AHU installations.
With a direct-drive plenum, the fan wheel is mounted directly on the motor shaft. There are no belts or sheaves and there are fewer bearings; direct-drive fans are much more reliable and require less maintenance than belt-drive fans. There are fewer moving parts, no belt-related drive losses, and less inlet or outlet obstructions. Direct-drive plenum fans are typically more efficient and much quieter than belt-drive plenum fans. Because the motor is in line (or parallel) with the direction of airflow through the AHU, the motor mounted behind the fan wheel does not restrict airflow, protrude from the side of the unit, or increase the unit width.
However, the AHU may need to be slightly longer to accommodate the motor mounted behind the fan wheel. This can be offset partially by using a fan array arrangement, which can add more redundancy to the unit operation. Depending on the location of the fan within the AHU, a plenum fan may be more efficient than a housed fan. A specific concern in health care facilities is the current prevalence of airborne pathogens that can be recirculated through AHUs. Because the airstream isn’t contained within the fan scroll and confined airway, pathogens can contaminate all the components that normally wouldn’t be in the airstream. These pathogens may not survive for very long on these surfaces, but people servicing the plenum components should take some precaution during the immediate time frame after unit shutdown.
The fan is selected to meet the requirement of the design airflow and the total pressure requirement. ASHRAE Standard 90.1-2016: Energy Standard for Buildings Except Low-Rise Residential Buildings provides the maximum fan-power requirement for HVAC systems based on the airflow rate and a variety of factors related to application and filtration level. Health care facilities usually have more stringent filtration requirements than some of the other commercial buildings, and the designers needs to ensure that the maximum fan-power selection incorporates the filter at about medium-loaded level.
The current edition of ASHRAE 90.1 incorporates a minimum fan efficiency grade (FEG) as described in AMCA Standard 205-10: Energy Efficiency Classification for Fans. Fans more than 5 hp will be required to have a minimum FEG of 67 and will need to operate within 10% of their peak efficiency. (This may not apply to packaged units, which are certified in their entirety). FEGs were formalized with the publication of AMCA 205 in 2010, and an AMCA Certified Ratings Program is now in place to provide third-party verification of FEGs as specified in AMCA Publication 211-13: Certified Ratings Program—Product Rating Manual for Fan Air Performance.
Once the design engineer has narrowed the fan selection to a list that meets the minimum FEG rating, the focus should be on actual power consumed. Because FEG ratings measure peak fan energy efficiency and not actual operating efficiency, their main value is in differentiating between different fan types. The higher the FEG rating of the fan, the more efficient it is. However, this does not speak to the efficiency of the fan and the motor and the variable frequency drive.
The use of fan arrays is becoming commonplace in AHU fan selection. It is favored in health care facilities because it adds a level of resiliency to the air handling system. The use of multiple fans will allow for redundancy in the fan selection when compared with using a single fan; in the event of a fan failure within the array, that fan can be blanked off and the AHU can still perform to maintain the required airflow condition.
Sound attenuators
The acoustic performance of the AHU is extremely important for a health care facility, especially for the units that are located near to acoustically sensitive patients in ORs, post-operative spaces, NICUs, auditory testing spaces, etc. It’s always important to know the maximum acceptable noise level for these specialized spaces to inform the AHU selection process. The engineer will need to work with the project’s acoustic consultant if there is a stringent noise requirement. Sometimes the AHU will need sound attenuators to meet the acoustic-performance requirements.
Good fan selection and the proper specification of the unit casing can reduce the need for sound attenuators and other costly noise-cancelling techniques. Fibrous acoustical lining that is exposed to the airstream is not recommended in health care facilities. Almost all health care AHUs have moisture proof lined surfaces that can resist microbial and mold growth; these generally do not assist in sound attenuation. The best way to minimize a fan’s sound level is to reduce the fan power; however, more efficient fans usually have the poorest acoustic performance. Oversizing the fan will give you better acoustic performance, but this is at the expense of fan efficiency.
The best engineering practice for acoustic design is to provide sound attenuators in the ductwork for those zones that require greater acoustical performance and to ensure the system has the necessary static pressure in those duct runs to compensate for the added pressure drop through the attenuators.
Coils
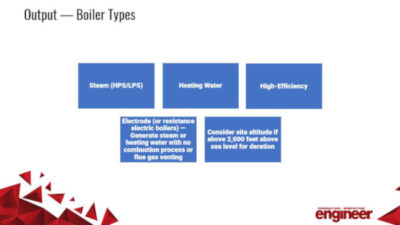
The coils section of the AHUs is used to cool, heat, and dehumidify air. Cooling and dehumidification can be provided by expansion of refrigerant (known as direct expansion, or DX, coils), or by chilled water. In drier climates, partial cooling also can be done by spray coils that reduce the dry-bulb temperature of the air but increase the air’s humidity level. The heat source for health care facilities can be from steam, hot water, or electricity.
Coil selection is an important part of the AHU design. Coil configurations are selected based on several criteria including coil face area, number of rows of tubes, tube diameter, number of fins, fin surface design, coil circuiting, and turbulators. Coil construction is based on tube material, tube and wall thickness, fin material and fin thickness, casing material, header type and material, and coil coatings. Coil selection is usually dependent on the type of unit selected; lower-tiered units usually have thinner coil materials to save cost.
Access
Access sections are key to the AHU design. Good design practice is to specify the access section after every major section of the AHUs, to permit ease of inspection and maintenance of the equipment and components. Access sections are often eliminated from AHUs due to space limitations or mechanical budget restrictions, but eliminating access sections can become problematic for maintenance, as each component within an air handler will require routine service, repair, or replacement many times over the life of the unit. Coils must be cleaned frequently to maintain proper heat transfer, and they must be accessible from both sides; therefore, coils should be specified with access sections at the front and back. An access section downstream of cooling coils also ensures condensation doesn’t get carried onto adjacent surfaces. Low velocity minimizes this, but budget-conscious projects rarely select AHUs with 450 feet per minute (fpm) or less coils. AHUs that are designed and installed without proper access to their components will neither be maintained properly nor perform as intended over the life of the unit.
Humidifiers
There are many methods for delivering humidification in AHUs; however, steam humidification is the predominant method in hospital design because steam is usually available from the hospital’s steam boiler plant. Ultrasonic or adiabatic humidification was not permitted in health care facilities until ASHRAE issued an addendum in 2016, to ASHRAE Standard 170. The original drawback from using adiabatic humidifiers was because of the threat of microorganisms and bacteria contamination in the airstreams by the water droplets from the process. Steam is a natural disinfectant, as most pathogens are immediately deactivated when exposed to temperatures as high as 100°C. Furthermore, steam is safe in terms of spreading contaminants, as it does not carry bacteria or other microorganisms.
The addition of moisture to airstreams depends entirely on psychrometrics of the system. The capacity of the air to absorb water depends, at a minimum, on the wet-bulb temperature and the absorption-distance chart. Mechanical designers should lean heavily on their psychrometric chart or other data to determine if a desired condition can be achieved.
It is vital to understand the chemical-treatment contents of the boiler plant’s steam when using building steam for humidification. If steam is used from a central plant’s steam source, be sure to verify that water treatment at the boiler plant does not jeopardize the steam purity, because this steam will be in direct contact with building occupants through the airstream. Typical treatment additives that should be avoided are those that contain “amines.” Steam-to-steam humidification should be considered if steam purity is poor in the hospital.
For hospital-system steam, humidification should be considered as the first option if the hospital already has a steam boilers plant. Steam distribution should be by injection into the airstream by steam grid humidifiers located in the AHUs downstream of the cooling coil. Steam-distribution rack assemblies should support the multiple steam manifolds. Provide access sections as a means of unobstructed clearance to lengthen the absorption distance downstream of humidifiers to allow complete absorption into the airstream. Otherwise, there will be ponding of moisture on surfaces and eventual mold and mildew growth.
Regardless of the humidification option selected, basis of design criteria need to be established. Minimum required criteria include:
Outside-air wet-bulb temperature: This is the ASHRAE-published weather data for the project area based on the project type. For hospital/medical projects use the 99.6% value, this should be used to calculate the mixed wet-bulb temperature that is used for sizing the humidifier.
Design indoor-space relative humidity (RH): For hospital/medical facilities, use ASHRAE Standard 170, Table 7.1. Increase the design criteria RH design value by 10% due to the accuracy of humidification controls. That is, where the criteria is used to maintain a minimum RH of 20%, select equipment based on a value of 30% RH.
Design indoor-space temperature: For humidification devices at AHUs, use the average return wet-bulb temperature from all spaces ahead of any return-air fan and prior to entering the unit. Where the humidification device is a booster humidifier, use the setpoint temperature within the space where the space humidistat is located.
Airflows: The quantities of outside, supply, and return air will be necessary to establish prior to humidifier selection.
Supply-air wet-bulb temperature: This is the supply air wet-bulb temperature upstream of the humidifier.
Garold “Gary” Hamilton is a senior vice president and health care practice lead at WSP. He was a 2015 40 Under 40 award winner.