NFPA 70-2017: The National Electrical Code (NEC) has many requirements that apply to designing electrical systems for health care facilities. It’s vital to understand the changes in the 2017 edition in order to stay code-compliant.
Learning Objectives:
- Understand NFPA 70 changes applicable to health care facilities.
- Learn about NFPA 99 and how it supplements Article 517 in NFPA 70.
- Know how to apply these code changes when designing health care facilities.
The health care construction industry is one of the most regulated industries in the United States. There are more than a dozen national, local, state, and government codes and standards that are applicable to the design, installation, maintenance, and performance of health care facilities. The most popular codes include NFPA 70 National Electrical Code (NEC), Article 517 Health Care Facilities; NFPA 99: Health Care Facilities Code; NFPA 101: Life Safety Code; NFPA 110: Standard for Emergency and Standby Power Systems; Facility Guidelines Institute (FGI), ASHRAE 170: American Society of Heating Refrigerating and Air-Conditioning Engineers Standard on Ventilation of Health Care Facilities; Center for Medicare and Medicaid Services (CMS); United States Pharmacopeia (USP), Chapter 797 Pharmaceutical Compounding—Sterile Separation and Chapter 800 Hazardous Drugs—Handling in Healthcare Settings; International Building Code (IBC); and The Joint Commission accreditation standards, just to name a few.
NFPA 70 Article 517 applies to the construction and installation of electrical systems in health care facilities that provide services to human life. NFPA 99 covers the performance of electrical systems in health care facilities. Health care facilities are covered in Article 517 in NFPA 70. Electrical systems are covered in Chapter 6 of NFPA 99.
New definitions in NFPA 70
There are new definitions in Article 517 of NFPA 70 that have design implications that need to be considered by the consulting-specifying engineer.
The governing body of the health care facility is “the person/s who has the overall legal responsibility for the operation of a health care facility.” The governing body establishes and identifies the patient care space categories in the health care facility based on the anticipated level of patient care and designates wet-procedure locations. The above areas of responsibility have many requirements that must be considered by the consulting engineer, including the number and type of receptacles and number of branch circuits in patient spaces, special protection against electric shock in wet-procedure locations, and loading on the alternate power source.
An invasive procedure is defined as “any procedure that penetrates the protective surfaces of a patient’s body and that is performed with an aseptic field (procedural site).” Not included in this category are special procedures such as the placement of peripheral intravenous needles or catheters used to administer fluids or medications, insertion of urethral catheters, and other similar procedures. What is important for the consulting engineer to understand about invasive procedures are what make certain spaces in a health care facility a Category 1 risk space. Category 1 spaces have special requirements in wiring, protection, and the type of the essential electrical system (EES) that supplies these spaces. NFPA 99 (Item A.6.7.5.1.3) recommends an automatic battery-operated lighting unit or system to provide minimal task illumination in invasive-procedure spaces.
A medical office is “a building or part thereof where the following occur: 1) examinations and minor treatments or procedures performed under the continuous supervision of a medical or dental professional; 2) only sedation or local anesthesia is involved and treatment or procedures do not render patients incapable of self-preservation under emergency conditions; and 3) overnight stays for patients or 24-hour operation are not provided.” What is important for the consulting engineer to understand is that there is a difference between a health care occupancy and a health care facility. All health care occupancies are health care facilities, but the opposite is not true. A health care occupancy is used to provide medical or other treatment or care simultaneously to four or more patients on an inpatient basis, where such patients are mostly incapable of self-preservation due to age, physical or mental disability, or because of security measures not under the occupant’s control. A hospital, for example, is a health care facility but can be of several different occupancies (health care, business, assembly, ambulatory, etc.). A medical office is a health care facility, but under NFPA 101 it would typically be a business occupancy.
Patient care spaces as defined in NFPA 70 are now aligned with the same definition in NFPA 99. A patient care space is “any space of a health care facility wherein patients are intended to be examined or treated.” There are four categories in health care facilities identified by the governing body based on 1) the anticipated level of patient care in any given space; and 2) the risk to the patient from procedures that will be performed.
Table 1 provides a distinction summary of patient care spaces, gives examples of these spaces, and discusses their design considerations as stipulated in NFPA 70 and NFPA 99.
NFPA 70-2017 “Type” classification
The 2017 version of NFPA 70 has now aligned the Type classification of the EES with NFPA 99. Type 1 and Type 2 EES are referenced in NFPA 70 Article 517.29 (Essential Electrical System Requirements for Hospitals and Other Health Care Facilities) and in Article 517.40 (Essential Electrical Systems for Nursing Homes and Limited Care Facilities), respectively. It is to be noted that the “type” terminology is also mentioned in NFPA 110 and applies to the emergency power supply system. The following paragraphs clarify what the type means as referenced in NFPA 70, NFPA 99, and NFPA 110.
NFPA 99, Item 6.7.1.2.4.1, requires that Type 1 and Type 2 EES power sources be classified as Type 10, Level 1 generator Class X, per NFPA 110. The type in NFPA 110 is the maximum time in seconds that the emergency power supply system (EPSS) will permit the load terminals of the transfer switches to be without power. The class in NFPA 110 is the maximum time in hours for which the EPSS is designed to operate at its rated load without being refueled. This means that power must be restored within 10 seconds, but the amount of time the EPSS is required to run without refueling is not defined in NFPA 110 and needs to be specified as required by other codes or by the authority having jurisdiction.
Figure 5: This diagram shows the difference between a Type 1 and a Type 2 essential electrical system.[/caption]
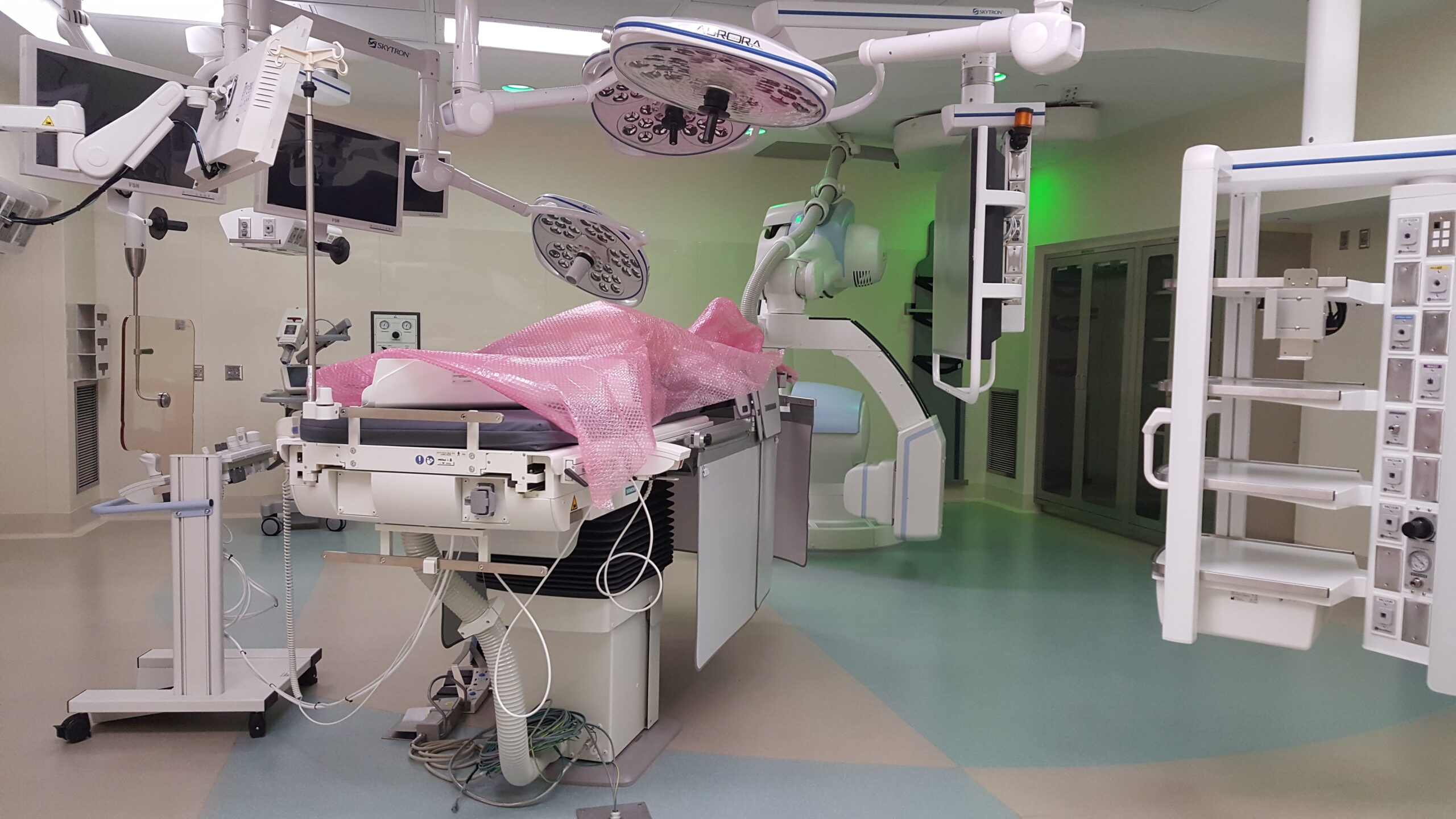
Figure 2: A hybrid operating room in a hospital—a Category 1 (critical care) space. All graphics courtesy: AECOM[/caption]
There are also notable changes in NFPA 70-2017 made to Article 700. Article 700.3.F now calls for an emergency system that relies on a single alternate source of power that will be disabled for maintenance or repair, to include a permanent switching means to connect a portable or temporary source of power, and be available for the duration of the downtime. Manual switching is allowed to be used in this case to switch from the permanent source to the portable source. Some health care facilities have multiple alternate power sources, such as generators connected in an N or N+1 configuration. In a two-generator scheme connected in parallel in N configuration and supplying 100% of the total essential load, either generator would comply with the above requirement in this case, if it can support the life safety system load by itself. The portable or temporary power-source connection could also be used to connect a portable load bank to comply with NFPA 110 periodic maintenance testing and loading requirements, which are mandatory for Level 1 and Level 2 standby and emergency power systems. See Figure 6.
Another important requirement has been added in NFPA 70 Article 700.10(D)(3) is fire protection for emergency (life safety) feeder circuit wiring for health care occupancies where patients are not capable of self-preservation, such as hospitals and ambulatory care occupancies. The code lists a number of options to comply with this requirement including installing life safety feeders in spaces that are protected by an approved fire-suppression system, using feeder cables that are a listed electrical circuit protective system, or encased in a minimum of 2 in. of concrete. As required by other codes, a water-based sprinkler system is typically provided in health care occupancies; however, the code stipulates that running feeders above a ceiling in an otherwise fully sprinklered building does not meet the requirement unless there are also sprinklers in the plenum space above the ceiling. Without proper consideration to the routing of feeders, this new requirement could have a very large financial impact on the installation. The consulting engineer might consider installing emergency feeders in areas that are typically fully sprinklered, such as vertically within electrical rooms or horizontally in areas without a suspended ceiling, and avoiding horizontal feeder runs above suspended ceilings that are not sprinklered, to avoid the additional cost of the other fire protection measures.
Another addition to Article 700 of NFPA 70 which is directly related to Article 517, is a new requirement for generator-control wiring. The article states that generator-control wiring installed between the transfer equipment and the emergency generators must be kept entirely independent of all other wiring and must be protected against fire in line with the fire protection measures listed above. Article 700.10(D) (3) now calls for continuous monitoring of the integrity of the generator-control wiring. Without this monitoring, an open circuit on the control wiring would go undetected and won’t be noticed until there is a power outage and the generator fails to start. This new requirement entails three elements: 1) continuous monitoring of generator signal circuits; 2) visual and audible annunciation; and 3) automatic transmission of an engine start signal and an alarm when a problem is detected. Several transfer switch manufacturers offer an easy solution for existing and new installations. Existing wiring does not need to be changed in this case, but additional circuit-communication modules would have to be added at both ends of the control wiring: at the generator and at the transfer equipment.
Article 517 of NFPA 70 has many design considerations for the consulting engineer designing health care facilities. These design considerations cover the wiring and protection of the electrical distribution system in patient care spaces and the EES in various health care occupancies.



