There are three considerations for working with existing smoke control systems in hospitals
Learning objectives
- Understand the primary types of legacy smoke control systems encountered in hospitals.
- Gain an understanding for how smoke control codes have changed over time.
- Develop strategies for addressing legacy smoke control systems as part of renovations and additions.
Hospital-based smoke control systems are a critical component of a facility’s life safety systems. Maintaining these systems in functional condition requires a basic understanding of the existing systems installed in a health care facility, including original design intent, major components and applicable regulatory requirements at the time of installation and those retroactively required based on current standards.
1. Individual air handlers with purge, evacuation sequences
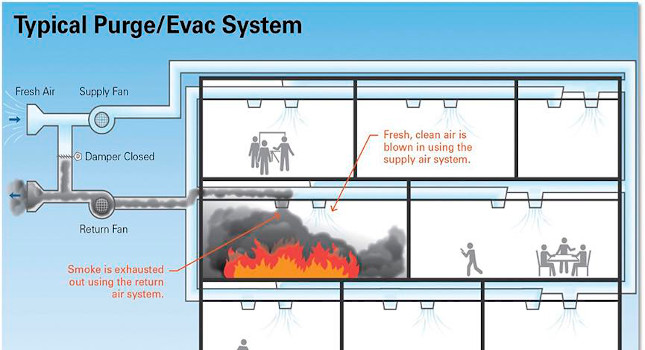
Many existing hospital air handling units dating back to the 1960s were designed and equipped with a means of switching from standard ventilation modes to a smoke emergency mode of operation, often referred to as either purge/evacuation or smoke vent. This system design was a common means of complying with either the NFPA 99: Health Care Facilities Code windowless inhalation anesthetizing requirements, the older model building code mechanical smoke vent requirements or, in some cases, both.
This typically consisted of a shift from modulated return and supply air flow to 100% exhaust via the return air system and a relief air section and 100% outdoor air via the supply air system. Where units were already 100% outdoor air and exhaust, the mode switch was typically an increase in air volume via fan speed or volume dampers and fully opening intake and relief dampers.
System performance was limited by the maximum air changes the existing ventilation system was designed to provide with a typical overall minimum of six air changes per hour based on older model building code language. In practice, using the ventilation system to flush areas with fresh outdoor air and pulling the contaminated air out via the return air system often provides marginal results.
In field testing using smoke bombs in individual spaces with the system operating in full purge/evacuation mode, smoke would mix thoroughly in the space and would take hours to remove entirely. Evaluating the necessity and efficacy of these systems and deciding prudent action to take based from the results of these actions is recommended.
Coordinated smoke vent systems
A more complicated version of the individual purge/evacuation AHU were coordinated purge/evacuation systems where AHUs serving entire zones, floors or buildings were programmed to act singularly. All AHUs in the coordinated system would respond to purge/evacuation or evacuation only, globally based on any initiating event in the entire system. These systems were sometimes referred to as engineered smoke control systems, typically designed to provide compliance with the pre-2000s model building codes for mechanical smoke vent systems.
Global system response was less common, possibly due to the complexity of coordinating these systems in pre-digital systems, the lack of direct language to this effect in older model codes and the impact these systems had on hospital operations due to singular detection events.
Coordinated zone pressurization systems
Found most commonly in high-rise hospital towers dating from roughly 2000 on (a major rewrite of the smoke control language in the 2000 edition of the International Building Code), a coordinated approach to smoke migration control and removal often using the hospital AHU ventilation system.
Buildings are divided into zones, most commonly a floor or smoke compartment and equipped with dampers on the supply and return/exhaust main trunks serving these zones. Smoke detected in any zone may initiate an evacuation sequence in the zone of origin and a pressurization sequence in the surrounding zones. Smoke is then isolated and removed from within the zone or compartment of origin, inhibited from movement by the relative pressure differential between the zones.
In practice, where a sufficiently high-pressure differential can be achieved, these systems are effective against smoke migration outside of the zone of origin and less effective at smoke removal as it was reliant on the same ventilation rates of the source system as noted previously.
Stair and elevator shaft pressurization systems
Many code-designated high-rise hospital structures were equipped with either smoke-proof enclosures — stair vestibules on each floor that are open to the outdoors or vestibules that are mechanically ventilated — or a mechanical pressurization system. Stair pressurization systems are typically dedicated fan systems ducted to pressurize either a series of vestibules or the stair itself. The stair is protected against smoke accumulation by the positive pressure differential, allowing its function as a safe egress path to be maintained.
Many stair and elevator shaft pressurization systems are equipped with a means of maintaining a set differential pressure by varying air volume at the fans or relieving air from the shaft. A minimum and maximum differential pressure are maintained to minimize smoke migration without resulting in excessive door opening and closing pressures.
Atrium purge and exhaust systems
Large open spaces in main entry areas were and still are a popular architectural design in hospitals. Where these openings communicated multiple floors’ egress paths, active smoke control systems were often required and installed. These typically consisted of a dedicated exhaust system drawing from the atrium ceiling and makeup air intake system of dampered louvers drawing outdoor air at low points in the atrium.
Due to the dedicated design nature of these systems, even before the more specific performance requirements laid out in the 2000 edition of the IBC, atrium smoke control systems are relatively effective compared to their nondedicated AHU-based counterparts.
2. Smoke control codes over time
It bears noting that NFPA 92: Standard for Smoke Control Systems is largely not referenced in this article except as a basis for testing standards for existing systems. This is due to other standards being the primary reference point for most legacy systems (e.g., NFPA 99 and the local state building codes).
Anesthetizing location systems: 1960 to 2012 — All hospitals under the jurisdiction of Centers for Medicare & Medicaid Services and/or a state agency adopting the NFPA codes, including NFPA 99 and NFPA 56: Standard for Fire and Explosion Prevention During Cleaning and Purging of Flammable Gas Piping Systems, are likely to have been required to provide active smoke control systems to serve all inhalation anesthetizing locations installed roughly from 1960 to the adoption of the 2012 edition of NFPA 99 by state and local authorities having jurisdiction and the adoption of the 2012 edition of NFPA 101: Life Safety Code by CMS.
This came from past editions of NFPA 56 and NFPA 99 back to the 1960 edition of NFPA 56, to the expansion of text in the 1978 edition of NFPA 56A: Inhalation Anesthetics. From the 1978 edition of NFPA 56A Section 3-1.1 to the 2005 edition of NFPA 99 Section 6.4.1, the code language remained largely the same. This required all windowless, inhalation, anesthetizing locations to be arranged to automatically vent smoke and products of combustion. In the 2012 rewrite of NFPA 99, this language was removed.
Vintage building smoke control systems: 1970s to 2000 — State building codes are, by their nature, more difficult to completely research with the numerous historical model code bases. However, from collected research in older building codes, active smoke control system references largely entered model code texts in the early to mid-1970s and were centered on high-rise structures and atriums. This would appear to correlate with the focus on high-rise fire safety of the same timeframe nationally.
The earliest specific language the author has found regarding active smoke management systems is from the 1975 edition of the North Carolina State Building Code, Section 521 for high-rise buildings. This was based on the National Building Code of Canada 1973 edition, and the NBC Measures for Fire Safety in High-Rise Buildings. Earlier editions of the building codes in North Carolina reference nonmechanical smoke control measures such as smokeproof vestibules for stairwells, but no active mechanical system requirements that the author has observed.
From 1975 through the 2000 edition of the IBC, there were references to smoke control systems to be installed in high-rise structures for general smoke management, in stair and elevator shafts and in open atrium whether in a high-rise structure or not. The specifics vary based on the model code and the year, but largely include the following up until 2000.
Between the 1970s and late 1980s, hospitals could be designated high-rise structures as low as three stories and 36 feet in height, requiring smoke venting via panels or windows or by using the mechanical air handling equipment to accomplish smoke removal on each floor. The specifications for these systems were limited, generally requiring that return and exhaust air be moved directly to the outside and the supply system providing 100% outdoor air at a minimum of six to 10 air changes per hour (e.g., 1978 North Carolina State Building Code, Section 506.5).
Most, if not all, elevator shafts were required to be pressurized such that two hours following a fire event, they would not contain more than 1% of contaminated air by volume.
Stairwells were required to be smokeproof (vestibules vented to the outdoors) or they were allowed to be pressurized meeting the same 1% contamination requirement after two hours as the elevator shafts.
In the late 1980s and 1990s, the high-rise threshold generally shifted to 75 feet, more detailed requirements were added for stairwell pressurization systems including specified air volumes and maximum differential pressures. Otherwise the smoke vent requirement language stayed much as it was. The term engineered smoke control system came into parlance roughly in the 1990s, but significant details on what was an acceptable engineered system were not mandated in the code until 2000.
In 2000, the IBC included a significant rewrite to the requirements for high-rise smoke control systems for general floors, stairs and elevator shafts under IBC Section 909. For general floor smoke management, pressurization across smoke barriers (zone pressurization) was designated as the primary compliance means. Specific and highly detailed requirements were laid out for zone pressurization, airflow method, exhaust method, stair and elevator shaft pressurization and atrium smoke control. IBC Section 909.6.1 included specific pressure differential requirements and IBC Section 909.6 pressurization method was the designated primary method of controlling smoke.
3. Approaching legacy systems in hospitals
There are several items to note for engineers working in hospitals that may be equipped with these systems.
Existing system analysis, documentation
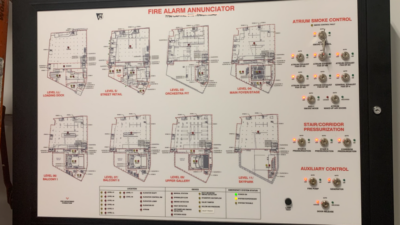
A complete inventory including location, service areas, major components, sequences of operation, access and controls should be developed for all existing smoke control systems. Equipment inventories, computerized maintenance management system data, local technician knowledge, fire alarm and building automation system point lists and user interface screens and, of course, flipping through old plan room drawings are all good resources for identifying existing systems. Be sure to field-check stair and elevator shafts and atriums for the existence of pressurization equipment.
Look for purge-evacuation and smoke vent sequences in 2012 and older AHUs serving anesthetizing locations. Check fire command centers and fire alarm control rooms for smoke control panels. Check any high-rise tower HVAC systems for evidence of smoke vent sequences in the ventilation systems and for zone pressurization in newer buildings, especially post-2000. Always field verify the physical condition and existence of systems identified from plans and other data sources.
Compliance requirements at time of construction
As important as understanding what is out there is, equally important is understanding what was and is required based on the original and current requirements for these structures. Knowing the dates of original construction or major renovation for each tower or building, the height and high-rise classification of each major separate structure, tower or atrium will allow you to determine the applicable codes and standards for the systems identified and for those that may be missing.
A useful clue on tower age are elevator inspection placards; these will often indicate the original installation date of the cab (which are not often replaced in their entirety) and may correlate to the original construction date.
From here, code research will be required to determine the specific editions of the local building codes, NFPA editions and state licensure requirements that were in place at the time of original construction or major renovation. Spots to focus on are the high-rise sections, nonflammable inhalation anesthetizing location requirements, stair and elevator shafts and open atriums.
Additionally, determining if structures would qualify as high-rise under the current requirements (typically 75 feet) is a good context point to determine if systems would be required under today’s codes or only under historical requirements.
Current system conditions
Once you have a clear picture of what systems exist and what they were and are required to do, physical testing and inspection is needed to verify baseline condition and performance. Thesesystems are highly prone to inadvertent debilitation, confirming whether the system is still functioning as it was intended will be a critical data point in future decision making on what to do with the system.
The first step should include visual inspection of the individual system components, fans, motors, belts, dampers, ducts, required to support the basic system functions. Documenting and addressing any physical deficiencies should occur before testing begins.
After the system is confirmed to be physically in place, point-to-point testing should be implemented to confirm each sequence step against the original system design. Additionally, performance testing should include verification of system-intended functions, checking differential pressures and air flow rates to confirm they fall within design parameters, required compliance thresholds and rational expectations.
Testing and inspections should be thoroughly documented including both the required and measured metrics and the reference design and compliance standards. This documentation helps greatly to substantiate existing system performance for future design decisions and authority having jurisdiction review and decision-making.
Modifying or replacing
When approaching a project affecting older facilities equipped with vintage, but still functional, smoke control systems, it can be tough to decide what direction to take. Maintain or expand the existing system, demolish and design a new retrofit system or something in between, these decisions can have major implications on cost and scope.
However, with good documentation and system baseline testing in hand, the process may be approached with more clarity and logic. Items to assess beforehand:
- What existing systems are present or may be affected by the project scope of work.
- The original design documentation and standards at the time of construction for these systems.
- The functional condition of these systems.
Good questions to ask are:
- Is a smoke control system still required in this facility type and, if so, what requirements are they and how do they differ from the existing system?
- Are the existing infrastructure systems capable of complying with modern requirements without major modification or replacement (e.g., are the existing fire alarm and mechanical control systems capable of UL 864 compliance)?
- Does the scope of the new work affect a sufficiently significant portion of the structure to warrant assessment against current code? This can go either way with respect to smoke control systems. In some cases, structures equipped with older systems would no longer require active smoke control if under current
Once sufficient clarity is achieved on the above aspects, a logical approach can be determined balancing the impact to the facility and patients, project scope of work, budget and overall compliance. It may be that the existing systems are too far gone to recover or the facility has evolved past their effective functionality.
Stair, elevator, atrium pressurization systems
Stairwell, elevator and atrium pressurization systems are relatively easy to maintain functionality and performance due to the simplicity of fan, louver, controls sequences and functional performance. Additionally, pressurizing these shafts is a highly effective means of minimizing smoke contamination of critical egress paths in hospitals.
Atrium exhaust systems are also relatively simple and effective smoke management systems. Maintaining these systems where found is recommended when possible and certainly where they remain a requirement from current or existing code.
Anesthetizing location smoke control systems
Anesthetizing location smoke control systems (simple purge-evacuation sequences for AHUs) are no longer mandated by most state AHJs where the 2012 or later edition of NFPA 99 has been adopted and no longer mandated via CMS referenced code text via NFPA 101-2012 and NFPA 99-2012. Individual state licensure rules may still contain references to anesthesia smoke control and should be confirmed as part of the decision-making process for these units.
Air handler-based purge-evacuation systems in the experience of the author are minimally effective in controlling smoke accumulation and present an often misunderstood and difficult to protect sequences of operation for facilities long-term. Without the current mandate for this function, a decision may be made to either maintain these sequences or switch to the more manageable and reliable shutdown response sequence.
Buildingwide egress and tenability systems
Determining an appropriate approach to these systems is inherently more difficult than stair-elevator pressurization, atrium exhaust and anesthesia locations due to the wider operational impact, relative complexity and broader code implications. Where existing systems rely on purge-evacuation sequences with existing AHUs, as is the case in anesthetizing location systems, this approach generally is less effective than a zone pressurization system relying on pressure differentials across smoke barriers.
Functioning and well-maintained zone pressurization systems may be highly effective in preventing smoke migration from the compartment of origin to adjoining areas. However, as previously noted, they are typically complex and where good documentation and testing practices are not in place, often found to be in dysfunctional condition.
It is always recommended to approach these systems in their entirety of original and/or current service area rather than through the lens of a renovation area barrier. Where a tower is equipped with a zone pressurization system, this consistent approach for the entirety of the tower should be maintained or if modified, done so globally rather than locally. Depending upon a structure’s overall height and the total percentage of renovation, it may be that a buildingwide smoke management system is no longer required. In such a case, designers may reconsider the necessity and benefits of maintaining existing systems.
Passive barriers and smoke control systems
Another common problem is what to do with existing purge-evacuation or zone pressurization systems using existing duct systems affected by modern renovations. In many cases, duct-mounted smoke dampers were omitted from penetrations of smoke barriers and shaft enclosures where the system was designed as part of an engineered smoke control system.
Language to this effect has been included since 2000 in IBC text where dampers would inhibit the operation of compliant smoke control systems designed to this code. During renovations of these older systems, especially before the aforementioned language existing, installing dampers in passive barriers such as smoke compartment boundaries and shafts is often mandated by code, but could result in duct system damage and inhibition of existing system operation where existing purge-evac sequences exist.
In this case, a good approach would be to assess the necessity and effectiveness of the existing system and decide whether advocating for maintaining the existing system without dampers or controlling dampers in coordination with the sequence is the better approach, or decommissioning the system and using the passive barrier approach is more beneficial.
In all cases, before making the decision to decommission, maintain or replace any existing smoke control system, consider having a discussion with the owner and local and state AHJ to confirm the solution. Most every edition of NFPA and building codes has had language requiring existing life safety systems to be maintained in place unless they exceed that which is required for new construction.AHJs would be the appropriate decision-makers to assist with determining whether smoke control systems ought to be maintained or replaced.