As health care projects become more patient oriented, human-centric lighting design and lighting controls are taking center stage

Learning Objectives
- Learn about three different lighting experiences in a health care environment.
- Understand how to apply human-centric lighting controls to health care projects.
- Observe the challenges in achieving human-centric lighting controls and corresponding solutions.
Lighting control insights
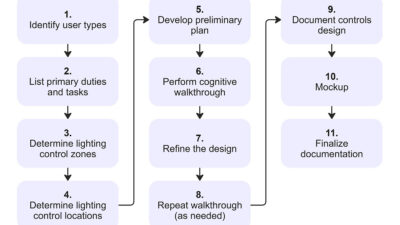
- When designing lighting control systems, it’s important for the electrical engineer or lighting designer to consider all aspects of use.
- Energy codes and standards challenge lighting designers to implement the most energy-efficient option for the health care project.
To achieve the best lighting control strategies, it is imperative to look at each type of space separately and define criteria that is useful for the design. For example, a health care environment involves a plethora of different programs and the individuality of each space affects the lighting control strategy dramatically.
![]() As an electrical engineer or a lighting designer start on a new project, they are usually faced with comments from clients and users about the importance of lighting controls in a health care environment. The ease of controlling lighting is imperative for a great patient experience.
As an electrical engineer or a lighting designer start on a new project, they are usually faced with comments from clients and users about the importance of lighting controls in a health care environment. The ease of controlling lighting is imperative for a great patient experience.
In some existing facilities, the lighting can be harsh and directional. The ability to control the lighting while in bed can be nonexistent. Patients can struggle to walk through a crowded room with the IV pole just to turn the lights on and off.
Human-centric lighting design could lead to a positive patient experience in health care facilities. As building designers embrace technology and the need for net zero, the careful balance between cost, comfort and energy efficiency is the way to the future. Simply providing a lighting controls solution that meets minimum code requirements might not be the best approach, especially when designing state-of-the-art health care facilities.

How human-centric lighting uses lighting controls
How can a lighting designer achieve a human-centric experience using lighting controls? The client and the users must be on board with the design and in tune with the future facility. A health care project involves the interactions of multiple experiences including the patient, visitor and staff experiences. Each experience type carries a diverse set of requirements from the code perspective, and also from the human or user’s side.
These requirements should be tailored to the needs of each facility. The complexity of the design requires the proper layering of lighting and lighting controls to achieve maximum comfort for the patient while maintaining a highly technical and functional space for the caregiver.
Let’s study each category individually:
Patient experience: It’s important for a patient to feel comfortable when coming into a hospital environment. Proper lighting design can play a key role in patient outcomes, which is augmented by the lighting control experience. When a patient has personal control, they can feel less stressed in an already-stressful situation. In fact, ANSI/IES RP-29-22: Recommended Practice: Lighting Hospital and Health Care Facilities reinforces the need for flexible patient controls to assure patient comfort and satisfaction.
Increasing patient satisfaction is one important metric hospitals look for to achieve the total performance score (TPS) managed and rated by The Centers for Medicare & Medicaid Services. A low TPS can reduce Medicare payments to a hospital due to poor satisfaction under the “person and community engagement domain” and due to frequent re-admissions. Body of evidence referenced by ANSI/IES RP-29-22 concluded that patient comfort also aids in faster healing and a quick turnaround. This in turn leads to better infection control as the patients’ stay in the hospital shortens.
Visitor experience: A visitor’s experience is similar, as the goal of controls for that category is to provide intuitive, easy-to-use controls. Providing care for a loved one should not come with the frustration of operating multiple keypads and complicated controls. Incorporating intuitive localized controls into the lighting design for the visitor zone provides localized lighting to the area without disturbing the patient’s sleep and respite. This helps reduce the trial-and-error efforts for a visitor to adjust the lighting in the visitor zone.
Staff experience: Staff controls can be used to help increase their efficiency and accuracy. For instance, lighting controls that turn on controlled beam task lights at staff work zones are strongly desirable. These controls should be clearly defined and located near their tasks as well as near the entrance to decrease the need for staff to find the proper switches. Touchless controls for task lighting are also strongly encouraged to reduce staff contamination as described in the ANSI/IES RP-29-22 Lighting Controls Systems section.

How to achieve these lighting control strategies
To achieve the best lighting control strategies, a health care case study will be used: Penn Medicine’s Pavilion at the Hospital of the University of Pennsylvania. The state-of-the-art facility was designed and constructed by the integrated project delivery (IPD) team PennFIRST, which included HDR, Foster + Partners, BR+A, L.F. Driscoll and Balfour Beatty.
The facility opened in October 2021 after six years of working through an IPD process. During the design — which involved the colocation of the team, including client, designers, engineers, construction managers, estimators and contractors — lighting controls were at the center of multiple in-depth conversations focused on patient experience and comfort. Each area was discussed with the users, client and contractors to achieve the best design solution possible.

Patient rooms
For the hospital, the patient room had to achieve maximum comfort: with zones for ambient illumination, patient reading, night light, charting, sink and visitor zones. The IPD team produced a solution that integrated all lighting controls via a bedside touchpad. The touchpad can do the following: control lighting and heating, ventilation and air conditioning (HVAC); achieve digital visual communication with the care team; enable patients to order food; control the TV; and enable communication with loved ones outside the facility.
The controls depended on a visual screen that was easy to read and understand, so patients have an intuitive interface without the need to learn modern technologies. Most lighting zones mentioned above could be controlled and dimmed from the touchpad individually. Each zone is shown on the app, so the patient doesn’t have to guess the appropriate zone.
From the touchpad, the patient has control over their environment and they can dim the different zones as desired to achieve the best scenario possible for their comfort. They can also control the shades, lowering and raising them as desired. The scenarios are unlimited and flexible so different lighting settings can be achieved when the patients want to watch TV, read, order food, communicate with the care team or just relax.
For the less savvy patients, the traditional integration with the nurse call system was also introduced to control patient-oriented zones, such as the reading and ambient zones. An “all off” button on the nurse call was also introduced in case the nurse leaves the room with some lights on.
The caregivers also control a given set of keypads at localized areas around the room. At the charting station, two buttons control the tight beam chart task light, to not disturb the patient and the uplight in case more lighting is needed. In addition, the bedside station controls the exam lighting, reading light for the patient, ambient illumination and uplights.
At the main entrance, a keypad is divided into two clear sections: the upper section offering easy access for the patients/visitors to control the ambient illumination and uplights, while the lower section allows caregivers to control the charting lights so they can see their way into the room without disturbing the patient with overhead lighting.
The visitor zone has its own keypad for local controls of the lighting in that zone, as well as control for the window shades. All buttons on the patient room keypads are properly labeled with a master raise and lower key to control the lights.

Lighting controls in patient corridors
Patient corridors are critical spaces, where multiple functions coexist. Patient corridors are used by visitors as wayfinding, for the circulation of patients and as a potential work zone for caregivers in case of emergency. The control system must accommodate each function.
The lighting in the space consists of a series of linear lights on the core wall and a wall wash on top of each patient room for wayfinding. The lighting control system schedules the lighting to go on at 100% level in the morning, until 7 p.m. when the linear lights gradually dim down to 30% and the wall washers dim down to 50%. This creates a comfortable, human-centric environment for the patients where they can sleep at night and avoid spill lighting into the rooms.
For the remaining hours of visiting time, there is still ample illumination above the patient bedrooms for proper navigation. In the case of clinical emergency at nighttime, overrides are provided at each nurses’ station using an intuitive touchpad. The caregivers then can attend to a patient in need of care, in the corridor with ample illumination.

Charting stations
Charting stations are also part of the corridor and they are intended for the caregiver to process information and medication locally. One charting station can monitor two rooms at the same time. A linear fixture with regressed lens was used to reduce light spill into the rooms. Each charting station lighting is controlled separately for maximum control and to avoid patient discomfort during quiet times.
The doors and windows into the patient rooms include smart glass for patient comfort. The glass can be controlled by the caregiver at the charting station, to turn the window and door separately. This ensures that the patient can keep their privacy with the door on opaque setting, while the caregiver can monitor the patient through the window on the transparent setting. The patient also has control of both the glass and window from inside the patient room unless the caregiver overrides that functionality.
Emergency life safety lighting in the corridors is controlled via a UL 924-rated device that ensures the lighting in the corridors are dimmed and controlled together with the regular lighting settings. The days of having dedicated noncontrolled emergency fixtures in a patient corridor are gone. The patient’s experience is a primary goal in ensuring their comfort, therefore controlling the spill light into patient rooms at night is critical.
Lighting control challenges
What are the challenges that designers face to achieve a more human-centric experience for a health care environment? Electrical engineers and lighting designers are faced with challenges due to updated, more stringent energy codes. Moreover, they are also challenged with an ever-changing environment of technologies and health care criteria.
The job of the designer is to assess those challenges and establish a set of priorities to meet client aspirations, project goals, budget and code.
Circadian rhythm entrainment
Due to the advancement of tunable white technology, circadian rhythm entrainment became a reality. Tunable white technology is the ability of changing the color temperature of a source following the black body curve by mixing two or more different color sources. Entrainment is a fundamental property of circadian systems by which the period of the internal clock is synchronized to the period of the entraining stimuli.
Research cited in the health and wellness section of ANSI/IES RP-29-22 reinforces the effects of entraining patient’s circadian rhythm on increasing patient outcomes, accelerating healing and creating a human-centric environment for the patient to overcome the harsh clinical environment. Tunable white technology research cited by the health and wellness section of ANSI/IES RP-29-20 also suggests the amelioration of the caregiver’s health and work environment especially for the ones that work late and night shifts.
However, tunable white technology comes with a slew of challenges to the lighting control system. There is currently little standardization of the technology which creates different comparative color temperature between different fixtures depending on binning. LED binning is a practice carried out to ensure high quality and consistency in the performance of LED light output and color. The technology is also still cost prohibitive in most health care projects and the cost is added to both the lighting fixtures and the lighting controls.
To overcome some of these challenges, it is recommended to put different fixture types on separate zones to avoid the difference in color temperature. This way each individual lighting type can be tuned separately to achieve the desired color temperature in the space. Another recommendation is to use the same manufacturer for the tunable white fixtures so the technology and the dimming rate, as well as color consistency, is the same.
Newer Digital Addressable Lighting Interface (DALI) protocols such as DALI DT8 and DALI-2 protocols also currently offer a solution for some manufacturers to provide a good standardization to follow the black body curve and provide another level of consistency.

Emergency lighting
As described in the case study, the future of health care lighting is through using controllable emergency lighting. To provide a human-centric comfortable solution, emergency lighting cannot be left on at night. This can be a burden to the budget, especially if every fixture is provided with a separate emergency module or if they need to be circuited to both the normal and the emergency circuits.
A suggested solution is to put long run fixtures on the same zone and circuit to use the same emergency module. Moreover, keeping the emergency lighting to the required minimum by code and by facility requirements can reduce cost and keep the project in budget. Some wireless lighting control systems can also be conducive since they reduce the amount of wiring.
However, one must keep in mind the requirements by NFPA 70: National Electrical Code, where some lighting control systems might not meet new emergency life safety requirements. It is also critical to consult with the client as some health care providers do not prefer wireless systems as they can cause electromagnetic interference with their systems and have batteries with short life spans which can also cause a maintenance issue.
Electromagnetic interference
Hospitals are a living structure of devices and equipment. With the advancement of newer wireless technologies, interference between different equipment in a hospital can create a serious challenge. Some occupancy sensors operate on the harmonics of newer real-time locating systems equipment and can interfere with them.
To use the advantages of wireless systems for a human-centric design, a careful investigation of the system frequency and its harmonics is crucial. If the project timeline permits, it is also encouraged to do a mock-up during the design phase with the various hospital and lighting equipment, which can lead to specifying the appropriate lighting control system early in the process.

Integration with BAS
A key element to achieving human-centric lighting controls is the capability to integrate multiple systems together. Because the building automation system (BAS) is often preferred by facility managers as an integration hub for a project’s major systems, it is crucial to integrate seamlessly with it.
Standard BAS protocol integration — such as BACnet, Modbus or others — is a feature in most lighting control systems. It is important to have a lighting control system that uses either no gateway with the BAS or minimal gateway. The former can be achieved using a lighting control system that uses the native BAS protocol.
Hence, control points between the two systems can be minimized and a direct two-way communication can be achieved. If the integration is successful, systems such as shades, smart glass, HVAC and others can be controlled from the lighting control system devices that already exist in the space. Reducing cost and consolidating keypads to lessen confusion in the space. In the case of a nurse call system, it can control lighting zones seamlessly as well.
A careful layout of the sequence of operations and how the system should operate makes the commissioning of the lighting system easier and less time consuming. This operational sequence should include the lighting zones and any integration between these different systems.

Expandable systems
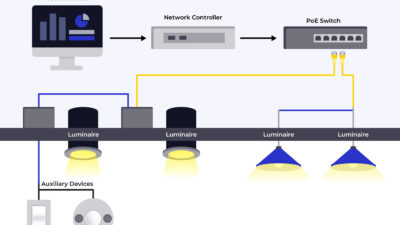
Because health care projects are projects that last for a long time and since a lot of upgrades can happen to the hospital, the lighting control system should be expandable and future proof. The ability for the systems to receive new products and upgrades is crucial. A distributed smart addressable system is a good approach.
Current lighting control systems are moving away from large, centralized lighting control panels toward more flexible plenum or fixture mounted lighting control modules. Each strategy comes with its own advantages and setbacks.
For instance, integrated controls in fixtures can cause a higher initial fixture cost but provides more flexibility in terms of future zoning. Fixture mounted controls and smart drivers are the way to the future so devices can be added to the lighting control grid seamlessly. A key approach to this is the standardization of both control modules and drivers.
Plenum-rated panels can be challenging in health care environments for maintenance above ceilings. This is why they are typically located in the corridors to avoid patient room shutdown. Plenum-rated panels are great to reduce cost and to zone multiple fixtures together in large areas such as corridors and lobbies. DALI and addressable systems represent about 70% of connected lighting systems according to the EU Joint Research Centre (JRC) and most European manufacturers have it as a standard offering. The technology is slowly making its way into the United States. If those are widely available, a system can be expandable.
The key to standardization is contacting manufacturers early in the process and communicating to them the importance of integrating specific drivers into their lighting fixtures. If the quantity is available, manufacturers will certainly be open to use such products.
Given the above-mentioned challenges, the best way to achieve a great design is to tailor it to the user’s needs. A strong understanding of what the client requirements are is crucial. Clear communication between the users and the design team is imperative. This communication can be visual, where different control scenarios can be shown or be in the format of a schedule or a diagram to indicate how zones are controlled and what type of devices are used.
Depending on the project timeline and delivery method, at least one meeting per phase for lighting controls is encouraged so the client can see the progress and comment on the changes. On larger immersive projects, the frequency of that review can increase to a weekly basis to ensure proper understanding of lighting controls by the client.
It is encouraged to show the different control scenarios to the client visually in the space. Renderings can be used to simulate them and to define how the space will look when built. This accelerates the sign-off process and eliminates future questions and requests for information.
It is also crucial to develop riser diagrams, schedules, details and sequence of operations that are reviewed by the client early in the process. The details and diagrams should be generic in nature to allow showing the intent without locking to a specific manufacturer and to make bidding easier. Documenting this information should be clear and consistent. It should also indicate which zones are dimmed, on emergency and the devices that control each zone.
Finally, a good lighting control system that provides a human-centric environment is critical for patient healing and eventually a better patient outcome. Specifying touchless controls, providing the patient with more controllability and circadian entrainment can promote faster healing, which can increase patient outcomes and reduce infection. This helps having a better return on investment as patient satisfaction and TPS scores increase. It also offers a viable solution for expanding in the future and adding the most current version of the lighting control system.