Designing air handling systems, especially for health care facilities, can be quite challenging given myriad constraints and choices for both the air handling units and their companion distribution networks
Learning Objectives
- Understand how the source and distribution portions of an air handling system work together.
- Learn about planning issues that influence air handling system decisions.
- Share lessons learned from a surgical suite pressurization problem.
There are several regulations that apply to the design, construction, operation and maintenance of air handling systems for health care facilities, the most important of which is ASHRAE Standard 170: Ventilation of Health Care Facilities. This standard addresses design criteria such as space dry bulb temperature, relative humidity, airflow rates and pressurization necessary to provide proper environmental control in clinical spaces.
Untangling all the codes and standards must be done to fully understand the constraints on a health care building’s air handling system design. These tools might include:
- ASHRAE Handbook
- ASHRAE HVAC Design Manual for Hospitals and Clinics
- ASHRAE Standard 62.1: Ventilation for Acceptable Indoor Air Quality.
- ASHRAE Standard 90.1: Energy Standard for Buildings Except Low-Rise Residential Buildings.
- ASHRAE Standard 170: Ventilation of Health Care Facilities.
- Facility Guidelines Institute.
- International Building Code .
- NFPA 99: Health Care Facilities Code .
- NFPA 101: Life Safety Code .
- State and local jurisdictions’ codes and guidelines.

Contamination control
There are several parameters that impact contamination control:
- The space dry bulb temperature and its companion relative humidity can affect how quickly particles of different sizes can be captured by air movement in a space.
- The quality of the supply air introduced into a space (meaning how much of the supply air is outdoor air instead of just recirculated air) can affect the dilution of particle counts in a space. In addition, the number of times per hour that a rooms’ air is changed out, defined as air changes per hour, can directly impact how clean a space becomes; dilution applies to spaces that have a design criterion of ISO 6 or higher (meaning dirtier).
- The purity of the supply air introduced into a space (meaning how much the supply air has been filtered and cleaned) can affect particle counts in a space; filtration and cleaning can take place at the air handling unit or within the room itself or both.
- The airflow pattern in a room is critical to moving air from clean to less clean areas, thereby keeping particles away from the breathing zones of vulnerable patients. In spaces like operating rooms where a design criterion of ISO 5 or lower (meaning cleaner) is the goal, a unidirectional airflow pattern must be developed as dilution doesn’t work for ISO 5 spaces or lower.
- And, finally, pressurization at the room level can help keep particles out of the patient space in the first place. It’s important to note that it’s difficult to guarantee that a space can be consistently negatively or positively pressurized without the use of an anteroom (sometimes referred to as an airlock). It’s also important to understand that a rooms’ porosity cannot be predicted — it must be measured after the room is built. As a result, designers must select system component capacities such that airflow rates can be adjusted during commissioning to achieve the desired differential pressure (usually about 0.03 inches w.g. with an alarm setpoint of 0.01 inches w.g.).
An air handling system is uniquely qualified to impact these parameters based on how both the AHU and its duct distribution are designed, built, operated and maintained.

Service areas
If we have a larger, multistory building, sometimes with institutional and business occupancies as defined by NFPA 101, how do we determine the system service areas? Do we provide a separate AHU for each floor? For each department? Do we provide a single set of interconnected systems for the entire building? What’s the optimum?
The most common criterion for segregation of system service areas would be extreme space temperature and relative setpoints such as those associated with a surgical suite. Another example would be departments, such as food service, that don’t require the same level of final filtration as other spaces in a hospital would require.
A guiding principle could be to provide identical systems including their AHUs unless one of the criteria noted above triggers a need to provide a unique system. Providing identical systems makes the design and documentation easier, makes furnishing and installing equipment much simpler and faster, makes commissioning more effective and minimizes the operation and maintenance for the owner over the life of the building. This can greatly reduce the life cycle cost of a system.
Another guiding principle could be to organize a stack of service areas to match a stack of smoke compartments and sprinkler water flow zones so that all the life safety systems are aligned.

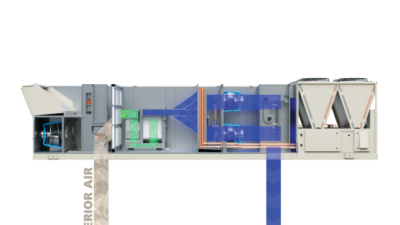
Basic all-air system configuration
An all-air variable air volume reheat system is the “go to” for hospitals. These systems are capable of dehumidification at low cooling loads because they consume a chilled water at a constant supply water temperature. They are also energy efficient in that they can reduce the volume flowrate of supply and return air as the cooling loads drop off.
AHUs work best when they are coupled with pressure independent duct distribution subsystems for both supply air and return air. This allows for more direct pressurization control at the room, suite or departmental level. Having pressure independent control of the airflows also eliminates the need to do any rebalancing of the medium-pressure supply or return air ductwork during renovation projects over the life of the building, significantly reducing the potential to disrupt clinical operations and substantially reducing the cost of renovations.
Another important design feature is connecting air handling systems together to provide an n+1 level of redundancy. This can be achieved by headering AHUs together in the fan room or by looping ductwork together out on the occupied floors. If a building can be provided with a minimum number of “families” of AHUs, then the total installed AHU capacity for a given n+1 level of redundancy can be minimized.
Headering air handling systems together by providing interconnecting “loops” of ductwork out on each floor has some advantages over headering the systems together in a fan room. First, headering ductwork together in a fan room means working with the largest ductwork in the system — clearly a disadvantage. Second, most fan rooms are too small and tend to be packed with all sorts of equipment, ducts, pipes and conduit — a little too congested to pull off headering of major ductwork effectively.
Connecting ductwork out on various floors can always be done with much smaller duct sizes and shorter lengths of ductwork that will result in lower material costs. A designer will need to consider protecting duct penetrations through smoke barrier walls, if required by NFPA 101, when choosing how to header the systems together.
A major responsibility of an air handling system beyond basic air conditioning (i.e., heating, humidification, cooling, dehumidification, filtering and cleaning) is to introduce outdoor air into occupied spaces. While dedicated outdoor air systems have become popular over the past several years, there are still many applications for which all-air systems are used to introduce outdoor air into occupied spaces.
When doing so, a designer has to consider whether to simply introduce the minimum amount of outdoor air during all hours of operation or to design a system that uses an airside economizer. The decision to employ an airside economizer requires some analysis. Energy codes including ASHRAE Standard 90.1 require that either an airside or waterside economizer be used.
In lieu of either of these two options, one could employ a heat recovery chiller. This heating, ventilation and air conditioning systemwide analysis can be complicated but should be done to thoroughly vet HVAC system options. Climate conditions will favor either an airside or a waterside economizer, especially if the climate is humid. But coincident heating and cooling loads during both the winter and the summer can make the use of heat recovery chillers a more energy efficient option than either type of economizer.
As an aside, airside economizers used for buildings such as hospitals in colder climates that need to be humidified can result in high humidification loads during the shoulder seasons of spring and fall and in higher humidification energy consumption over the whole year. Providing minimum outdoor air in all air systems eliminates the damper control problems commonly found with economizers and, in colder climates, minimizes the risk of stratification and coil freezing problems.


Air handling system calculations
It’s important to recognize that air handling systems are calculation-intensive. Space heating and cooling loads need to be prepared. How the air handling systems are headered together will determine how the space heating and cooling loads will be “zoned” so that diversity can be synced up with the system service areas. Ventilation schedules that capture the amounts of outdoor air, supply air and exhaust air required to meet various codes and standards, as well as the program requirements of a building, must be prepared.
It’s important to note that the “minimum” amount of outdoor must be selected using the following criteria:
- Any minimum air change rates found in states’ hospital licensing acts.
- The rates stipulated by ASHRAE Standard 62 and/or 170.
- The amount of outdoor air necessary to offset the amount of exhaust leaving the building.
Furthermore, the amount of outdoor air will be affected by how infiltration/exfiltration is estimated to be moving through the buildings’ envelope. All of these values will result in a set of system airflow rates for both the summer and the winter that can be captured in simple diagrams that become useful for visualizing full and part load and seasonal airflow movement through the system
It’s also important to note that these seasonal system flow diagrams will ensure that a design engineer thinks about how much lower the supply airflow rates will be during the winter than during the summer, thereby ensuring that reheat loads/energy can be estimated properly. Reheat energy is the Achilles’ heel of an all-air system, especially in a hospital application (this is what makes the use of heat recovery chiller so effective).
Then psychrometric calculations must be prepared. These calculations will focus on the “low side” of the cooling coil, which is to say the cooling coil leaving dry bulb and wet bulb temperatures. In any system in which you need to satisfy both a space dry bulb temperature and a space relative humidity simultaneously, the latent load must be addressed first and then the supply air temperature must be adjusted to subsequently meet the dry bulb temperature criteria. This means that the final supply air flow rate and commensurate temperature difference between the space and supply air can only be determined psychrometrically after the latent load has been satisfied.
Psychrometric calculations should be prepared for humidification such that if direct injection steam is used, then the commensurate heating of the supply air can be accounted for. Conversely, if adiabatic humidification is used, then the commensurate cooling of the supply air can be accounted for.
Fan power also must be assessed. This calculation will need to be done continuously throughout the early design phases to gauge how basic design criteria such as the speed of the air through the cooling coil will affect pressure drop and therefore the demand for power. Estimating the fan energy index has gotten a little more complicated than the early Standard 90.1 equations so understanding the nuances are critical study sessions for designers. It’s also important to consider operating “standby” AHUs during normal operation to further reduce the power demand by all the air handling systems.
Definitions
Contamination control: managing air quality in a space by limiting viable and nonviable particle including bacteria, virus and fungi as well as mitigating odors, all of which is in the domain of design engineers.
Environmental control: heating, humidification, cooling, dehumidification, air filtering and air cleaning
Infection control: managing the health of patients and their families as well as staff, all of which is in the domain of health care workers.