Incorporating pandemic response design into design/build hospital project
WSP USA Inc., formerly Leach Wallace Associates, was commissioned to provide full mechanical, electrical and plumbing design services for the Penn State Health Lancaster Medical Center to be constructed on a greenfield site in East Hempfield Township, Lancaster County, Pennsylvania.
The project delivery method was enhanced design assist with the construction manager and all major trade partners under contract at the start of schematic design phase working together with the architecture and engineering team, owner and other partners to meet the project schedule and target construction cost.
The goal of the project was speed to market within a target value cost. Project deliverables were aligned with procurement and installation schedules such that early design packages for major equipment, prefabricated central utility and electrical gear were issued before the completion of the hospital permit documents. This process required advance planning and anticipation of building program requirements and infrastructure capacities to develop early procurement packages in advance of completion of the full design.
The project design began in fall 2019 and design was scheduled to be completed by September 2020. The COVID-19 pandemic started in earnest in March 2020 and persisted throughout the rest of the year. The original hospital program included a limited number of isolation spaces within the emergency department and two airborne infectious isolation rooms in each patient care unit for 14 patient spaces for treatment of patients with highly infectious airborne illness.
This program was a typical approach for a community hospital setting, but as the pandemic set in throughout the late spring and summer it was clear to Penn State Health and the project team that additional considerations for pandemic response to this and future airborne pathogens was necessary.
WSP was tasked with developing a plan to incorporate provisions to allow for conversion of an entire patient care unit of 24 patient beds and a dedicated 10-bay observation unit in the emergency department for pandemic response. This would provide a total 46 patient treatment spaces that could be used for pandemic response.
This design was to incorporate required infrastructure such that these spaces could be converted within a few days into pandemic isolation units without the need of additional equipment, temporary air scrubbing equipment or exterior temporary ductwork. The fifth floor south wing was selected for the pandemic surge unit.
The team identified several different approaches for creating pandemic treatment spaces using increased ventilation rates, direct exhaust and additional filtration. The design approaches were as follows:
- Create an entire isolation patient care unit with ASHRAE 170: Ventilation of Health Care Facilities compliant AII rooms with 12 air changes per hour, required pressure differential and monitors and 100% exhaust through dedicated isolation exhaust system. The patient care unit common areas and support spaces would also be exhausted through dedicated systems and the entire unit would have a negative pressure relationship to the rest of the facility.
- Provisions for a pandemic surge unit would consist of a single patient care unit to be converted into a temporary pandemic surge unit with negative-pressure, 100% exhausted patient rooms, though not fully ASHRAE 170 compliant AII rooms (rooms have 12 ACH but may not meet minimum pressure differential to be classified as permanent AII rooms). Patient rooms would be exhausted through dedicated isolation exhaust system and common areas and support spaces would be served by conversion of return air systems to 100% exhaust purge mode through return air duct system and fans. AHUs would operate at 100% outside air to avoid any cross-contamination of air streams. The surge unit would have negative pressure relationship to adjacent spaces and have fixed pressure monitors for tracking of suite pressurization.
- Provisions for providing pandemic negative pressure patient rooms with standard airflow and converting patient room return air systems to provide negative pressurization to the corridors and use return air system in 100% exhaust purge mode with HEPA air filtration of the exhausted air stream. Common areas and support spaces would be served by conversion of return air systems to 100% exhaust through return air duct system and fans with high-efficiency particulate air filtration of exhaust stream.
- The emergency department observation suite would be converted to 100% exhaust through dedicated exhaust system to provide negative pressurization for temporary pandemic treatment. This space would have fixed pressure monitors for tracking of suite pressurization.
Due to the accelerated project design schedule, all the major equipment including, electrical distribution gear, central utility plant, major air handling equipment and hospital structural design had already been released to the construction manager and trade partners for procurement and fabrication.
Each option was evaluated for impact on the building infrastructure systems and equipment that was already in fabrication to determine how the systems and equipment could be modified or supplemented to serve pandemic response requirements. The proposed design approaches required increased air exchange rates, dedicated exhaust systems and corresponding make up outdoor air, which have significant impact on air handling equipment capacities, duct riser sizes and central plant capacity. The following was the impact of each approach:
- Isolation patient care unit: This would have required an additional dedicated air handling unit, exhaust fan system and duct riser as well as significantly reducing the redundant chiller water capacity in the central plant, which may have required the installation of an additional chiller.
- Pandemic surge unit: This option could use the air handling equipment currently in fabrication with modifications to the supply fans, heating and cooling coil capacities and modifications to unit controls strategies. Additional isolation exhaust system capacity could be achieved by enlarging the planned two fan exhaust array to a three fan system and providing a larger duct riser. Additional ductwork and control dampers would be provided to allow for system switchover between normal and pandemic surge operation. This approach limited the impact on the central chilled water plant and did not necessitate the need for additional central plant equipment.
- Pandemic negative pressure patient rooms: This option was not preferred by the health system because it did not provide additional ventilation to the patient rooms and dedicated exhaust path for contaminated air from the patient rooms. This option could be implemented without modifications to the air handling equipment or ductwork risers through automatic temperature control sequence changes.
- Emergency department observation unit: This option required the installation of an additional dedicated isolation exhaust fan system and modifications to the AHU heating and cooling coil capacities as well as control system modifications.
After evaluation of the infrastructure impacts, the pandemic surge unit approach was selected to provide the highest level of pandemic isolation and safety while controlling the potential modifications to the existing infrastructure systems and procurement and fabrication schedules. Each patient room would be fully exhausted at 12 ACH and under negative pressure to the corridor with nonpatient care areas and support spaces exhausted through the return air system operating as 100% exhaust in purge mode (see Figure 3).

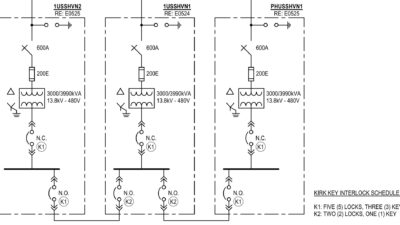
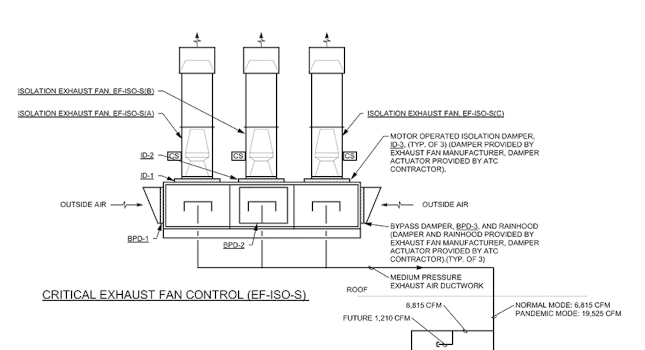
The AHU would be operated as 100% outdoor air to prevent any cross-contamination with supply air stream. The additional outdoor air flow required the design of additional cooling and heating capacity in the unit to allow for operation in any season. The originally designed isolation exhaust system was enlarged with the addition of a third fan and new dedicated exhaust riser to the fifth floor pandemic unit (see Figure 4).

All patient care areas in the unit would be exhausted through the dedicated isolation exhaust system. A system of automatic control dampers and specialized control sequences was provided to allow the facility to switch the heating, ventilation and air conditioning from standard operating mode to pandemic mode within a few hours (see Figure 5).
Once systems were switched over to pandemic operation, the test, balance and commissioning teams will verify and adjust the systems for pandemic operation. The HVAC systems have been provided with heating and cooling capacity to allow for pandemic operating at any time of year and could remain in operation indefinitely. Once the pandemic was over, the air handling equipment could be cleaned and the space could be returned to normal operation using standard supply and return air arrangement.

Vital building stats
Owner: Penn State Health
Project: Penn State Health Lancaster Medical Center, East Hempfield Township, Lancaster County, Pennsylvania
Description: 345,000 square feet, six-story 156 bed community hospital, aboveground parking structure and adjoining 60,000-square-foot ambulatory care building
Architect: HKS
Construction manager: Barton Mallow/Alexander Building Construction (Joint Venture)